Peculiarities of the structure of the human nose: only about the most important things. Clinical anatomy of the nose
23. Nasal cavity: the bony basis of its walls, communications.
The nasal cavity, cavum nasi, occupies a central position in the facial part of the skull. The bony nasal septum, septum ndsi osseum, consisting of a perpendicular plate of the ethmoid bone and a vomer attached below to the nasal ridge, divides the bony nasal cavity into two halves. In front, the nasal cavity opens with a pear-shaped aperture, apertura piriformis, bounded by the nasal notches (right and left) of the maxillary bones and the lower edges of the nasal bones. In the lower part of the pyriform aperture, the anterior nasal spine, spina nasalis anterior, protrudes forward. Through the posterior openings, or choanae, the nasal cavity communicates with the pharyngeal cavity. Each choana is bounded on the lateral side by the medial plate of the pterygoid process, on the medial side by the vomer, above by the body of the sphenoid bone, and below by the horizontal plate of the palatine bone.
The nasal cavity has three walls: upper, lower and lateral.
Top wall The nasal cavity is formed by the nasal bones, the nasal part of the frontal bone, the cribriform plate of the ethmoid bone and the lower surface of the body of the sphenoid bone.
Bottom wall The nasal cavity consists of the palatine processes of the maxillary bones and the horizontal plates of the palatine bones. Along the midline, these bones form the nasal ridge, to which is attached the bony nasal septum, which is the medial wall for each half of the nasal cavity.
Lateral wall The nasal cavity has a complex structure. It is formed by the nasal surface of the body and the frontal process of the maxilla, the nasal bone, the lacrimal bone, the ethmoid labyrinth of the ethmoid bone, the perpendicular plate of the palatine bone, the medial plate of the pterygoid process of the sphenoid bone (in the posterior section). Three nasal conchae protrude on the lateral wall, located one above the other. The superior and middle are parts of the ethmoidal labyrinth, and the inferior turbinate is an independent bone.
The turbinates divide the lateral part of the nasal cavity into three nasal passages: upper, middle and lower.
Superior nasal passage, medtus nasalis superior, is limited above and medially by the superior nasal concha, and below by the middle nasal concha. This nasal passage is poorly developed, located in the back of the nasal cavity. The posterior cells of the ethmoid bone open into it. Above the posterior part of the superior nasal concha there is a sphenoid-ethmoid recess, recesus sphenoethmoidalis, into which the aperture of the sphenoid sinus opens, apertura sinus sphenoidalis. Through this aperture the sinus communicates with the nasal cavity.
Middle nasal passage, medtus nasalis medius, is located between the middle and inferior nasal concha. It is significantly longer, higher and wider than the top one. The anterior and middle cells of the ethmoid bone, the aperture of the frontal sinus through the ethmoid funnel, infundibutum ethmoidale, and the semilunar cleft, hiatus semilundris, leading into the maxillary sinus open into the middle nasal meatus. The sphenopalatine foramen, foramen sphenopalatinum, located behind the middle turbinate, connects the nasal cavity with the pterygopalatine fossa.
Lower nasal passage, meat us nasalis inferior, the longest and widest, is limited above by the inferior nasal concha, and below by the nasal surfaces of the palatine process of the upper jaw and the horizontal plate of the palatine bone. The nasolacrimal canal, canalls nasolacrimalis, begins in the orbit, opens into the anterior section of the lower nasal meatus.
The space in the form of a narrow sagittal fissure, limited by the septum of the nasal cavity on the medial side and the nasal turbinates, makes up the common nasal passage.
In the front part of the skull there are cavities - voids, which are called paranasal sinuses. They act as resonators, thanks to which the mass of the head bones is reduced. Each sinus It communicates with the nasal cavity through the anastomosis - a narrow connecting passage. There are several types of paranasal, or paranasal sinuses, differing from each other in location, size, and structure.
Common to all paranasal sinuses
The anatomy of the nose and paranasal sinuses is especially actively formed during the first 5 years of life. Together with the paranasal sinuses, they form a single functional system.
All paranasal sinuses have walls that are dotted with numerous openings. Connective tissue cords, nerves, and blood vessels. However, through these same holes in the cavity the following can penetrate:
- pus,
- toxins,
- pathogenic flora,
- cancer cells spreading to the orbital area, pterygopalatine fossa, etc.
Due to the fact that the structure and physiology of the nose and paranasal sinuses allows for the possibility of pathogen traffic, the development of secondary diseases and the occurrence of complications after a seemingly harmless infection of an individual sinus are often observed.
Functions
One of the main tasks of the sinuses is considered to ensure the safety of the brain, eye sockets, facial nerves, arteries and veins. The anatomy of the paranasal sinuses normally implies the possibility of unhindered drainage of constantly produced mucus, the physiological function of which is to neutralize pathogens. The mucus is drained through the anastomosis, which must be open for this, and moves towards the exit thanks to the ciliated epithelium, covered with many cilia.
With the beginning colds mucus production increases.
However, in the case of significant swelling of the mucous membrane and blockage of the anastomosis, exudate accumulates in the cavities. The reason for this may be:

In addition to the protective function, there are:
- resonator, thanks to which an individual voice timbre is formed,
- respiratory (during nasal breathing, air circulates freely through the nasal passages, is moistened and warmed),
- olfactory (the task is performed thanks to the epithelial tissue that recognizes odors).
Anatomical abnormalities
The paranasal sinuses are diverse and different people their number and shape may vary. So, for example, according to statistics, 5% of people are completely absent. In addition, topographic relationships may be disrupted, thickening or thinning of the walls of bone tissue, on the surface of which there may also be congenital defects. Such anomalies occur in the late phase of prenatal (intrauterine) development.
Common anatomical anomalies include frontal and asymmetry. And in rare cases, there is a complete absence of the maxillary cavity and the division of the maxillary sinuses in half by a bone septum.

This division can occur both vertically (front and back) and horizontally (top and bottom).
More common is cracking of the upper wall of the maxillary sinus, which communicates with the inferoorbital canal or orbital cavity. The concavity of the facial wall, combined with the protrusion of the nasal wall into the lumen of the sinus, threatens the penetration of the needle under the cheek when attempting to puncture.
Anatomy and physiology also depend on the genetic factor, which can cause deformation of the facial and cerebral skeletons, as well as on metabolism.
For all sinuses in the paranasal region, the presence of fissure passages in communication with surrounding formations (dehiscence) is considered abnormal. For example, due to the occurrence of dehiscence:
- the ethmoidal labyrinth sometimes communicates with the frontal and, orbital, cranial fossae;
- the gap in the lateral wall of the main sinus contributes to the contact of its mucosa with the dura mater (brain) of the middle cranial fossa, with the pterygopalatine fossa, the superior orbital fissure and the optic nerve, the cavernous sinus and the internal carotid artery;
- thinning of the wall of the sphenoid sinus can lead to contact with the abducens and trochlear nerves, with the branches of the oculomotor and trigeminal nerves.
Maxillary (maxillary) sinuses
Paired caves, which are located in the thickness of the bone. In an adult, the volume of each can reach 30 cm 3 (max), but the average volume is about 10 cm 3. In volumetric form it resembles a triangular pyramid. Its three walls stand out:
- The superior (orbital) is the thinnest of the three, which is especially noticeable in its posterior section. Often it is in these places that gaps appear, and sometimes bone tissue is completely absent. Inside the wall, the canal of the infraorbital nerve passes from the infraorbital foramen. If the canal is absent, the nerve and accompanying blood vessels are adjacent to the mucosa. However, if inflammatory processes occur with this arrangement, the likelihood of intraorbital and intracranial complications increases.
- Lower (cave floor) - located near the back of the alveolar process (that is, near the upper jaw), so it sometimes happens that the sinus is separated from the four posterior upper teeth only by soft tissue. This proximity increases the risk of sinus inflammation due to odontogenic damage.
- The inner wall (also known as the lateral wall of the nasal cavity) normally corresponds to the middle and most of the lower nasal passages. In the posterior region of the semilunar notch under the middle part of the nasal concha, the maxillary sinus opens through this wall into the nasal cavity. Everywhere, except for the lower sections, this wall is thin enough to allow therapeutic punctures to be made through it.
The paired maxillary sinuses often differ in volume, while both conchas (right and left) have bays (small additional depressions): alveolar, palatine, zygomatic, frontal.

Frontal (frontal) sinuses
They are paired cavities that are located in the thickness of the frontal bone, namely, between the plates of the scales and the orbital part. The right and left shells are usually separated by a thin partition. However, due to the nature of the formation, options are possible when:
- the partition is shifted to the left or right, which sometimes causes a significant difference in the size of the shells,
- the septum may have openings that connect the frontal sinuses,
- cavities may be absent on one or both sides,
- the sinus can extend to the frontal scales, as well as to the base of the skull along with the perforated plate of the ethmoid bone.
The frontal sinus communicates with the concha of the nasal cavity through the frontonasal canal. Its outlet is located in the anterior part of the middle nasal meatus.
The frontal turbinates become a continuation of the anterior cells of the ethmoidal labyrinth, therefore, in the event of inflammation of one formation, the infection often spreads to the other.
- The anterior wall is the place through which the sinus is pierced or opened. The orbital nerve exits through the supraorbital notch.
- The lower wall is the thinnest of all, which makes it easier for infection to enter the orbit from the frontal concha.
- The brain wall, through which infection can penetrate into the anterior cranial fossa, it separates the conchae from the frontal lobes.
Lattice Maze

A collection of thin-walled cells consisting of bone tissue. Their average number is about 7-8 pieces, but the number can vary from 2 to 15. The cells are arranged in 3-4 rows, conventionally divided into front, rear and middle. They are located in the unpaired symmetrical ethmoid bone - in the notch of the frontal bone. The posterior cells contact the canal through which the optic nerve passes (sometimes it passes directly through them). Often the ethmoid labyrinth reaches the most distant cavities of the facial skeleton, bordering on vital organs.
The labyrinthine mucosa is innervated by the nasociliary nerve, a branch of the ophthalmic nerve. In this regard, many diseases that occur with damage to the ethmoid labyrinth are accompanied by pain. Due to the fact that the olfactory filaments pass in the tight canals of the bony cribriform plate, when edema develops due to compression, smell disturbances are common.
Sphenoid (main) sinus
 Due to its location in the sphenoid bone (behind the ethmoid labyrinth above the nasopharyngeal vault and choanae), the main sinus has a second name - the sphenoid. In an adult, this sinus is divided into right and left non-communicating parts, which in most cases do not coincide in size and have independent exits into the nasal passage. A total of five cavity walls are described:
Due to its location in the sphenoid bone (behind the ethmoid labyrinth above the nasopharyngeal vault and choanae), the main sinus has a second name - the sphenoid. In an adult, this sinus is divided into right and left non-communicating parts, which in most cases do not coincide in size and have independent exits into the nasal passage. A total of five cavity walls are described:
- Front. It consists of two parts: nasal and ethmoidal, which corresponds to the posterior cells of the ethmoidal labyrinth. The thinnest anterior wall smoothly passes into the lower one, facing the nasal cavity. There are small round holes in it, through which the main sinus communicates with the nasopharynx. They are located at the level of the end of the superior concha of the nose.
- Rear. The frontally located wall is less than a millimeter thick (with large volumes of the sinus), which creates a risk of damage during operations.
- Upper. Corresponds to the bottom of the sella turcica, in which the optic chiasm (wrapped in the arachnoid membrane) and the pituitary gland are located. In the case of inflammation of the sphenoid sinus, it often spreads to adjacent formations, sometimes affecting the olfactory pathways or even the anteromedial surface of the frontal lobes of the brain.
- Bottom. Thick (about 12 mm) wall corresponding to the arch of the nasopharynx.
- Lateral. These walls border directly on the neurovascular bundles, which are located on the sides of the sella turcica. They can both absorb the optic nerve canal and come into contact with it. Through the wall at the border with the cavernous sinus and optic nerve, infection can enter these formations.
Along with the listed sinuses, the pterygopalatine fossa, located behind the tubercle of the lower jaw, should be mentioned. Its clinical significance is great, since if the nerves located in the fossa are involved in the inflammatory process, neuralgic syndromes of the facial part occur.
Sinus inflammation: types and symptoms
 Depending on which sinus the inflammatory process occurs in, there are:
Depending on which sinus the inflammatory process occurs in, there are:
- sphenoiditis - inflammation affects the sphenoid sinus,
- sinusitis - the maxillary cavities are affected,
- frontal sinusitis – frontal areas are involved,
- ethmoiditis - the process occurs in the cells of the ethmoid labyrinth.
Inflammation of the mucous membrane can affect one or more sinuses at once. This inflammatory process occurs in different forms:
- acute form with pronounced symptoms,
- recurrent – with less pronounced repetition of signs of acute inflammation,
- chronic.
The chronic form of the inflammatory process, which most often affects the maxillary sinuses and slightly less frequently the frontal sinuses, lasts about 2-3 months, even if therapeutic measures are used. Signs of a chronic process include:
- Nasal discharge of purulent, mucous, watery or mixed consistency.
- Difficulty breathing due to blockage of the nasal passages.
- Sore throat and reflex cough arising from swelling of mucous masses in the back of the throat.
- Headaches, noted mainly in the nose, forehead and eyes.
- Impaired olfactory function.
- The growth of polyps from the paranasal sinuses into the nasal passages.
Unlike children, adults are more likely to experience a viral infection of the nasal mucosa, which spreads to the sinuses. Less commonly, blood diseases and dental conditions are the cause. The odontogenic factor is significant when the maxillary sinuses are affected. A viral infection, against the background of a “busy” immune system, can be accompanied by a bacterial factor, most often in the form of staphylococci, which can be activated.
Normally, microorganisms and microparticles, when inhaled, passing through the nasal cavity along with the air, enter the caves of the sinuses, where the ciliated epithelium captures them and neutralizes them to form mucus that is excreted. This mechanism can be disrupted by the curvature of various bone formations with anatomical deformation of the shells, as well as unfavorable factors affecting protective properties epithelium: dry air, tobacco smoke, chemical burns, tissue atrophy and necrosis, depressed state of the immune system, etc. Edema can also occur as a consequence of an allergic reaction.
 Some of the most common general symptoms of sinus inflammation include:
Some of the most common general symptoms of sinus inflammation include:
- runny nose with thick greenish discharge and pus,
- headache, which intensifies with changes in pressure, when tilting the head, pressing on areas in the area of the nasal sinuses, as well as a feeling of fullness in these areas,
- condition of nasal congestion,
- increase in body temperature to 38C,
- morning and night cough.
Due to congestion, a person begins to breathe through his mouth and speaks in a nasal voice. In this case, there is often an unpleasant odor from the mouth.
With sinusitis, headaches associated with a pathological increase in intracranial pressure are one of the main symptoms. Pain in the forehead and sinuses can be pulsating or squeezing, which is typical primarily for the acute form. In addition to the above signs, the following is noted:
- decreased sense of smell (or loss of it),
- lacrimation and fear of light,
- sometimes – swelling of the upper eyelid or cheek.
In the chronic course of the disease, secretions flow down the wall of the pharynx, causing a night cough. In the mornings and evenings, there is a characteristic pain radiating to the area of the eye sockets. When pressing on the inner corner of the eyes, the pain spreads to the entire face.
Treatment of inflammation
Treatment of inflammation is carried out using conservative or surgical methods, depending on the indications. Conservative methods involve removing swelling of the mucous membrane, destroying pathogens, creating conditions for the removal of mucus and organizing the patency of the sinus mouth.
When treating the acute form without the need to remove cysts, polyps, or eliminate deviated septum, the following is used:
- vasoconstrictors - to relieve swelling,
- local antibiotics – for purulent inflammation,
- antiseptic solutions in combination with rinsing through a puncture of the most convenient and thin wall,
- oil preparations for moisturizing dry mucous membranes, eliminating crusts,
- saline solutions when washing to moisturize and normalize exudate drainage.
The “Cuckoo” method for sinusitis
 Lavage is used only if there are no disturbances in the structure of the anastomosis, provided there is normal circulation of fluid through the nasal cavity. It is performed without anesthesia. The patient lies on his back. A catheter is inserted into one nostril to deliver medication, and a tube with a vacuum pump to pump out fluid is inserted into the other. During the procedure, the patient pronounces the onomatopoeic “ku-ku”, which gives the name to the method, to prevent the medicine from entering through the throat into the respiratory tract. When administering the medicine, a slight pressure is created to facilitate the flushing of exudate. When treating sinusitis, 5 sessions are usually prescribed.
Lavage is used only if there are no disturbances in the structure of the anastomosis, provided there is normal circulation of fluid through the nasal cavity. It is performed without anesthesia. The patient lies on his back. A catheter is inserted into one nostril to deliver medication, and a tube with a vacuum pump to pump out fluid is inserted into the other. During the procedure, the patient pronounces the onomatopoeic “ku-ku”, which gives the name to the method, to prevent the medicine from entering through the throat into the respiratory tract. When administering the medicine, a slight pressure is created to facilitate the flushing of exudate. When treating sinusitis, 5 sessions are usually prescribed.
Sometimes rinsing is combined with laser treatment, which is used to relieve swelling.
Flushing with a sinus catheter
Sinusitis can be treated without a puncture using the drug “Yamik”. To flush the patient, catheters are inserted through which high and low pressure is created (for this, an air cylinder is connected). Through one catheter, the contents of the sinuses are pumped out, and through the other, a medicinal solution is supplied. The procedure is performed under local anesthesia.
Cyst
The cyst is detected using radiography. Without it, patients hardly notice the tumor until it reaches a significant size, comparable to the volume of the sinus. In this case, symptoms characteristic of sinusitis begin to appear: headaches, a feeling of fullness, difficulty with nasal breathing. A cyst occurs when the ducts of the mucous gland are disrupted, causing mucus to accumulate in the spherical capsule. It can only be eliminated surgically after determining its exact location using CT and MRI:
- The classic method involves an incision in the wall under the upper lip, which is associated with long-term scarring and frequent subsequent relapses of sinusitis.
- The endoscopic method is performed using an endoscope with a camera through the anastomosis, which eliminates traumatic complications.
Fungal infection
 Fungal inflammation is not considered rare. The fungus affects one sinus or several at once.
Fungal inflammation is not considered rare. The fungus affects one sinus or several at once.
People at risk are HIV-infected and diabetics, and the likelihood of infection increases in people:
- conducting local treatment with steroids,
- regularly taking antibiotics,
- using drug therapy that leads to suppression of the immune system,
- who have undergone radiotherapy and chemotherapy due to cancer.
The inflammatory reaction is most often provoked by fungi of the genera candida, mucor, aspergillus, and rhizopus.
In this case, the symptoms of a fungal infection are similar to a bacterial infection. The course of the disease can vary from slow development to rapid growth fungal formations with severe manifestations. An accurate diagnosis is first established using radiological images, and then it is clarified by histological and mycological analyses. In case of fungal infection, antifungal drug treatment is most often combined with surgical intervention, aimed at removing polyps from the sinuses.
Features of inflammation in children
90% of all cases of sinus inflammation in children are bacterial in nature. Due to the fact that at this age there are a large number of variants of manifestations, sometimes difficulties arise with diagnosis. For inflammation in newborns, diagnosis is based on:
- cough,
- smell from the mouth,
- switch to mouth breathing,
- blocked nasal passages.
A specific symptom may include swelling of the eyelids and/or displacement towards the eyeball, which is associated with the location of the ethmoid sinus near the eye sockets, which in infants are separated from the sinus by a wall that is not yet fully formed. These manifestations are observed against the background of general symptoms: decreased appetite, tearfulness, and poor sleep. Older children may additionally complain of pain and swelling in the eye area. They also experience nasal congestion, followed by purulent mucous discharge.
Nasal cavity, cavitas nasi, is divided by the nasal septum, septum nasi, into two almost symmetrical parts.
The nasal septum is divided into: the membranous part, pars membranacea, the cartilaginous part, pars cartilagines, and the bony part, pars ossea.
Most of the cartilaginous part of the septum is formed by the cartilage of the nasal septum, cartilago septi nasi, an irregular quadrangular plate. The posterior margin of the cartilage is wedged into the angle formed by the perpendicular plate of the ethmoid bone and the vomer; in this case, the upper parts of this edge are attached to the anterior edge of the perpendicular plate, and the lower ones - to the anterior edge of the perpendicular plate, and below - to the anterior edge of the vomer and to the anterior parts of the nasal crest of the horizontal plate of the palatine bone and the anterior nasal spine of the body of the upper jaw.
The most narrowed part of the cartilage is the posterior process (sphenoid bone), processus posterior (sphenoidalis). The anteroinferior edge of the septal cartilage reaches the medial peduncle of the greater cartilage of the nasal wing, the anterosuperior edge reaches the inner surface of the dorsum of the nose in the suture area between the nasal bones.
The base of the nasal septum, which separates the nostrils, is called the movable part of the nasal septum, pars mobilis septi nasi.
In the nasal cavity, a distinction is made between the vestibule of the nasal cavity, vestibulum nasi, covered from the inside by the skin of the external nose extending through the nostrils, and the nasal cavity itself, cavitas nasi, lined with mucous membrane.
The vestibule of the nasal cavity, vestibulum nasi, is separated from the nasal cavity proper by a small protrusion - the threshold of the nasal cavity, limen nasi, formed by the upper edge of the lateral leg of the large cartilage of the nasal wing.

In the anterior sections of the nasal cavity itself, a small protrusion is distinguished - the nasal ridge, agger nasi. It follows from the anterior end of the middle concha to the threshold of the nasal cavity. Posterior to the nasal ridge is the vestibule of the middle meatus, atrium meatus medii.
The nasal cavity is divided into paired nasal passages. The superior nasal passage, teatus nasi superior, is limited by the superior and middle turbinates. The middle nasal passage, meatus nasi medius, is enclosed between the middle and inferior nasal concha. The lower nasal passage, meatus nasi inferior, is located between the inferior turbinate and the lower wall of the nasal cavity. The common nasal meatus is located between the medial surfaces of the turbinates and the nasal septum. The part of the nasal cavity lying behind the posterior ends of the turbinates is called the nasopharyngeal meatus, meatus nasopharyngeus.
The bones surrounding the nasal cavity are air-bearing and contain the paranasal sinuses, sinus paranasales. The latter communicate with the nasal passages: the maxillary sinus, sinus maxillaris, the frontal sinus, sinus frontalis, the middle and anterior cells of the ethmoid bone, cellulae ethmoidales mediales et anteriores, - with the middle nasal passage through the ethmoidal funnel, infundibulum ethmoidale, and the semilunar cleft, hiatus semilunaris; the posterior cells of the ethmoid bone, cellulae ethmoidalis posteriores, - with the upper nasal passage and the sphenoid sinus, sinus sphenoidalis, - with a common nasal passage at the level of the upper passage through the aperture of the sphenoid sinus, apertura sinus sphenoidalis.
The nasolacrimal duct, ductus nasolacrimalis, bounded by the lacrimal fold, plica lacrimalis, the lacrimal membrane, opens into the lower nasal passage.
Under the mucous membrane of the lower wall of the anterior section of the common nasal passage, 1.5-2.0 cm posterior to the nostrils, there is the upper opening of the incisive canal, canalis incisiuus, containing blood vessels and a nerve.
Correspondingly, at the posterior end of the middle turbinate, under the mucous membrane, there is a sphenopalatine foramen, foramen sphenopalatinum, through which vessels and nerves pass to the mucous membrane of the nasal cavity.

In the anterior sections of the nasal cavity, the mucous membrane is a continuation of the skin of the vestibule of the nasal cavity gradually passing into it; in the posterior sections, the mucous membrane through the posterior openings of the nose - choanae, passes into the mucous membrane of the pharynx and soft palate.
In the mucous membrane of the nasal cavity, as well as the paranasal sinuses, there are mucous glands, the size, shape and number of which vary in different parts of the nasal cavity. There are especially many glands in the mucous membrane of the respiratory region of the nose - these are the nasal glands, glandulae nasales.
A large number of blood and lymphatic vessels pass through the submucosa, while in the area of the middle and lower conchae there is a dense network of small vessels that form the cavernous venous plexus of the conchae, plexus cavernosi concharum. In the antero-inferior parts of the cartilaginous septum of the nose on the mucous membrane, posterior and above the mouth of the incisive canal, canalis incisivus, there is sometimes a small hole leading into a blindly ending canal running from front to back - the vomeronasal organ, organum vomeronasale. On the lateral side it is limited by the vomeronasal cartilage, cartilago vomeronasalis.
The mucous membrane of the nasal cavity is divided into respiratory and olfactory areas. The part of the nasal mucosa lining the superior conchae and the free sides of the middle conchae facing the nasal septum, as well as the corresponding upper part of the nasal septum, belongs to the olfactory region, regio olfactoria. The endings of the olfactory nerves, nn, also lie in the mucous membrane of this area. olfactorii. The rest of the mucous membrane of the nasal cavity is included in the respiratory region, regio respiratoria.
Innervation: mucous membrane of the anterior section - n. ethmoidalis anterior (from n. nasociliaris) and rr. nasales interni (from n. infraorbitalis); posterior section - n. nasopalatinus and rr. nasales posterior, superior et inferior (branches of ganglion pterygopalatinum n. maxillaris).
Blood supply: a. sphenopalatina (from a. maxillaris), aa. ethmoidales anterior et posterior (from a. ophthalmica).
Venous blood flows from the nasal mucosa along v. sphenopalatina in plexus pterygoideus. Lymphatic vessels from the nasal mucosa approach the nodi lymphalici submandibulares and submentales.
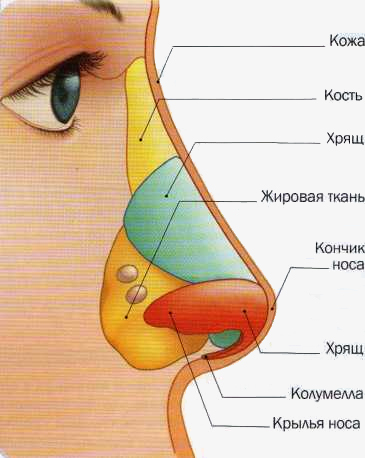
Rice. 1. The basis of the cartilaginous part of the external nose is the lateral cartilage, the upper edge of which borders on the nasal bone of the same side and partially on the frontal process of the upper jaw. The upper edges of the lateral cartilages form a continuation of the dorsum of the nose, adjoining in this section the cartilaginous part of the upper parts of the nasal septum. The lower edge of the lateral cartilage borders the greater wing cartilage, which is also paired. The large wing cartilage has medial and lateral crura. Connecting in the middle, the medial crura form the tip of the nose, and the lower parts of the lateral crura form the edge of the nasal openings (nostrils). Between the lateral and greater cartilages of the nasal wing, sesamoid cartilages may be located in the thickness of the connective tissue, different shapes and magnitude.
The wing of the nose, in addition to large cartilage, includes connective tissue formations from which the posterior sections of the nasal openings are formed. The inner sections of the nostrils are formed by the movable part of the nasal septum.
The outer nose is covered with the same skin as the face. The external nose has muscles that are designed to compress the nasal openings and pull down the wings of the nose.
The blood supply to the external nose is provided by the ophthalmic artery (a. ophthalmicа), dorsal nasal (a. dorsalis nasi) and facial (a. facialis) arteries. Venous outflow occurs through the facial, angular and partially ophthalmic veins, which in some cases contributes to the spread of infection in inflammatory diseases of the external nose to the sinuses of the dura mater. Lymphatic drainage from the external nose occurs in the submandibular and superior parotid lymph nodes. The motor innervation of the external nose is provided by the facial nerve, and the sensory innervation is provided by the trigeminal nerve (I and II branches).
The anatomy of the nasal cavity is more complex. The nasal cavity is located between the anterior cranial fossa (above), the orbits (laterally) and the oral cavity (below). In front, the nasal cavity communicates with the nostrils external environment, behind with the help of the choana - with the nasopharynx area.
There are four walls of the nasal cavity: lateral (lateral), internal (medial), upper and lower. The most complex structure is the lateral wall of the nose, formed by several bones and bearing the nasal turbinates. Its bone formations include the nasal bones, the upper jaw, the lacrimal bone, the ethmoid bone, the inferior nasal concha, the vertical plate of the palatine bone and the pterygoid process of the sphenoid bone. On the side wall there are three longitudinal projections formed by shells. The largest is the inferior nasal concha; it is an independent bone; the middle and superior conchas are outgrowths of the ethmoid bone.
The lower wall of the nasal cavity (bottom of the nasal cavity) is actually the hard palate; it is formed by the palatine process of the upper jaw (in the anterior sections) and the horizontal plate of the palatine bone. At the anterior end of the bottom of the nose there is a canal that serves for the passage of the nasopalatine nerve (n. nasopalatinus) from the nasal cavity to the oral cavity. The horizontal plate of the palatine bone limits the lower parts of the choanae.
The inner (medial) wall of the nasal cavity is the nasal septum (Fig. 2). In the lower and posterior sections it is represented by bone formations (the nasal crest of the palatine process of the upper jaw, the perpendicular plate of the ethmoid bone and an independent bone - the vomer). In the anterior sections, these bone formations are adjacent to the quadrangular cartilage of the nasal septum (cartilage septi nasi), the upper edge of which forms the anterior section of the nasal dorsum. The posterior edge of the vomer limits the choanae medially. In the anteroinferior section, the cartilage of the nasal septum is adjacent to the medial processes of the large cartilage of the nasal wing, which, together with the skin part of the nasal septum, form its movable part.
Rice. 2. Nasal septum 1. Lamina cribrosa 2. Crista sphenoidalis 3. Apertura sinus sphenoidalis 4. Sinus sphenoidalis 5. Ala vomeris 6. Clivus 7. Pars ossea 8. Pars cartilaginea 9. Septum nasi 10. Lamina medialis processus pterygoidei 11. Processus palatineus Maxillae 12. Crista nasalis 13. Canalis Incisivus 14. Spina Nasalis Anterior 15. Cartilago alaris Major 16. Cartilago vomeronasalis 17. Cartilago Septi Nasi 18. Cartilago Nasi Lateralis 19. Vomer 20. Pecess US Posterior 21. OS NASALE 22. Lamina Perpendicularis Ossis Ethmoidalis 23. Crista gali 24. Sinus frontalis
Rice. 2. The upper wall of the nasal cavity (roof) in the anterior sections is formed by the nasal bones, the frontal processes of the upper jaw and the partially perpendicular plate of the ethmoid bone. In the middle sections, the upper wall is formed by the ethmoid bone (lamina cribrosa), in the posterior sections - the sphenoid bone (the anterior wall of the sphenoid sinus). The sphenoid bone forms the upper wall of the choana. The cribriform plate is pierced big amount(25-30) openings through which the branches of the anterior ethmoidal nerve and the vein accompanying the anterior ethmoidal artery and connecting the nasal cavity with the anterior cranial fossa pass.
The space between the nasal septum and the turbinates is called the common meatus. In the lateral sections of the nasal cavity, corresponding to the three nasal conchae, there are three nasal passages (Fig. 3). The lower nasal passage (meatus nasi inferior) is limited from above by the inferior nasal concha, from below by the bottom of the nasal cavity. In the anterior third of the lower nasal meatus, at a distance of 10 mm from the anterior end of the concha, there is an opening of the nasolacrimal canal. The lateral wall of the lower nasal passage in the lower sections is thick (has a spongy structure), closer to the place of attachment of the inferior nasal concha, it becomes significantly thinner, and therefore puncture of the maxillary sinus (correction of the nasal septum) is carried out precisely in this area: at a distance of 2 cm from the anterior end of the lower shells
 Rice. 3. Nasal cavity 1. Bulla ethmoidalis 2. Concha nasalis inferior 3. Concha nasalis media 4. Concha nasalis superior 5. Apertura sinus sphenoidalis 6. Sinus sphenoidalis 7. Meatus nasi inferior 8. Meatus nasi medius 9. Bursa pharyngealis 10. Meatus nasi inferior 11. Tonsilla pharyngealis 12. Torus tubarius auditivae 13. Ostium pharyngeum tubae 14. Palatum molle 15. Meatus nasopharyngeus 16. Palatum durum 17. Plica lacrimalis 18. Ductus nasolacrimalis 19. Labium superius 20. Vestibulum nasi 21. Apex nasi 2 2. Limen nasi 23. Agger nasi 24. Dorsum nasi 25. Processus uncinatus 26. Hiatus semilunaris 27. Radix nasi 28. Aperturae sinus frontalis 29. Sinus frontalis
Rice. 3. Nasal cavity 1. Bulla ethmoidalis 2. Concha nasalis inferior 3. Concha nasalis media 4. Concha nasalis superior 5. Apertura sinus sphenoidalis 6. Sinus sphenoidalis 7. Meatus nasi inferior 8. Meatus nasi medius 9. Bursa pharyngealis 10. Meatus nasi inferior 11. Tonsilla pharyngealis 12. Torus tubarius auditivae 13. Ostium pharyngeum tubae 14. Palatum molle 15. Meatus nasopharyngeus 16. Palatum durum 17. Plica lacrimalis 18. Ductus nasolacrimalis 19. Labium superius 20. Vestibulum nasi 21. Apex nasi 2 2. Limen nasi 23. Agger nasi 24. Dorsum nasi 25. Processus uncinatus 26. Hiatus semilunaris 27. Radix nasi 28. Aperturae sinus frontalis 29. Sinus frontalis
Rice. 3. The middle nasal passage (meatus nasi medius) is located between the inferior and middle nasal concha. Its lateral wall is represented not only by bone tissue, but also by a duplication of the mucous membrane, which is called “fontanella” (fontanelles). If the middle turbinate is partially removed, a semilunar cleft (hiatus semilunaris) will open, bounded in the anteroinferior parts by a bone plate (uncinate process), and in the posterosuperior parts by a bone vesicle (bulla etmoidalis). In the anterior sections of the semilunar fissure, the mouth of the frontal sinus opens, in the middle sections - the anterior and middle cells of the ethmoid bone sinuses, and in the posterior sections there is a depression formed by the duplication of the mucous membrane and called the funnel (infundibulum), which ends with a hole leading into the maxillary sinus.
The superior nasal passage (meatus nasi superior) is located between the superior and middle nasal concha. The posterior cells of the ethmoid bone open into it. The sphenoid sinus opens into the sphenoethmoidal recess (recessus sphenoethmoidalis).
The nasal cavity is lined with mucous membrane, which covers all the bone sections of the walls, and therefore the contours of the bone section are preserved. The exception is the vestibule of the nasal cavity, which is covered with skin and has hairs (vibrissae). In this area, the epithelium remains stratified squamous, as in the area of the external nose. The mucous membrane of the nasal cavity is covered with multirow cylindrical ciliated epithelium.
Depending on the structural features of the nasal mucosa, the respiratory and olfactory sections are distinguished. The respiratory department occupies the area from the bottom of the nasal cavity to the middle of the middle turbinate. Above this border, the ciliated columnar epithelium is replaced by a specific olfactory epithelium. The respiratory section of the nasal cavity is characterized by a large thickness of the mucous membrane. Its subepithelial section contains numerous alveolar-tubular glands, which, according to the nature of the secretion, are divided into mucous, serous and mixed. The respiratory part of the mucous membrane is characterized by the presence in its thickness of cavernous plexuses - varicose veins with a muscular wall, due to which they can contract in volume. The cavernous plexuses (corpus cavernosa) regulate the temperature of the air passing through the nasal cavity. Cavernous tissue is contained in the thickness of the mucous membrane of the inferior turbinates, located along the lower edge of the middle turbinate, in the posterior sections of the middle and superior turbinates.
In the olfactory region, in addition to the specific olfactory epithelium, there are supporting cells that are cylindrical, but lack cilia. The glands present in this section of the nasal cavity secrete a more liquid secretion than the glands located in the respiratory part.
The blood supply to the nasal cavity is carried out from the system of external (a. carotis externa) and internal (a. carotis interim) carotid arteries. The sphenopalatine artery (a. sphenopalatina) originates from the first artery; passing through the main palatine opening (foramen sphenopalatinum) into the nasal cavity, it gives off two branches - the posterior nasal lateral and septal arteries (aa. nasales posteriores laterales et septi), providing blood supply to the posterior sections of the nasal cavity, both the lateral and medial walls. The ophthalmic artery originates from the internal carotid artery, from which branches of the anterior and posterior ethmoidal arteries arise (aa. ethmoidales anterior et posterior). The anterior ethmoidal arteries pass into the nose through the cribriform plate, the posterior ones through the posterior ethmoidal foramen (foramen ethmoidale post.). They provide nutrition to the area of the ethmoid labyrinth and the anterior parts of the nasal cavity.
The outflow of blood occurs through the anterior facial and ophthalmic veins. Features of blood outflow often determine the development of orbital and intracranial rhinogenic complications. In the nasal cavity, particularly pronounced venous plexuses are present in the anterior sections of the nasal septum (locus Kilsselbachii).
Lymphatic vessels form two networks - superficial and deep. The olfactory and respiratory areas, despite their relative independence, have anastomoses. Lymphatic drainage occurs in the same lymph nodes: from the anterior sections of the nose to the submandibular, from the posterior to the deep cervical.
Sensitive innervation of the nasal cavity is provided by the first and second branches of the trigeminal nerve. The anterior part of the nasal cavity is innervated by the first branch of the trigeminal nerve (anterior ethmoidal nerve - n. ethmoidalis anterior - branch of the nasociliary nerve - n. nasociliaris). The nasociliary nerve from the nasal cavity penetrates through the nasociliary foramen (foramen nasociliaris) into the cranial cavity, and from there through the cribriform plate into the nasal cavity, where it branches in the region of the nasal septum and the anterior sections of the lateral wall of the nose. The external nasal branch (ramus nasalis ext.) between the nasal bone and the lateral cartilage extends onto the dorsum of the nose, innervating the skin of the external nose.
The posterior sections of the nasal cavity are innervated by the second branch of the trigeminal nerve, which enters the nasal cavity through the posterior ethmoidal foramen and branches in the mucous membrane of the posterior cells of the ethmoid bone and the sinus of the sphenoid bone. The second branch of the trigeminal nerve gives off the nodal branches and the infraorbital nerve. The nodal branches are part of the pterygopalatine ganglion, but most of them pass directly into the nasal cavity and innervate the posterosuperior part of the lateral wall of the nasal cavity in the region of the middle and superior nasal concha, the posterior cells of the ethmoid bone and the sinus of the sphenoid bone in the form of rr. nasales.
Along the nasal septum, a large branch runs from back to front - the nasopalatine nerve (n. nasopalatinus). In the anterior parts of the nose, it penetrates through the incisive canal into the mucous membrane of the hard palate, where it anastomoses with the nasal branches of the alveolar and palatine nerves.
Secretory and vascular innervation comes from the superior cervical sympathetic ganglion, the postganglionic fibers of which penetrate into the nasal cavity as part of the second branch of the trigeminal nerve; parasympathetic innervation is carried out through the pterygopalatine ganglion (gang. pterigopalatinum) due to the nerve of the pterygoid canal. The latter is formed by the sympathetic nerve, originating from the superior cervical sympathetic ganglion, and the parasympathetic nerve, originating from the geniculate ganglion of the facial nerve.
Specific olfactory innervation is carried out by the olfactory nerve (n. olfactorius). Sensitive bipolar cells of the olfactory nerve (I neuron) are located in the olfactory region of the nasal cavity. The olfactory filaments (filae olfactoriae), extending from these cells, penetrate into the cranial cavity through the cribriform plate, where, connecting, they form the olfactory bulb (bulbus olfactorius), enclosed in the vagina formed by the dura mater. The pulpy fibers of the sensitive cells of the olfactory bulb form the olfactory tract (tractus olfactorius - II neuron). Next, the olfactory pathways go to the olfactory triangle and end in the cortical centers (gyrus hippocampi, gyrus dentatus, sulcus olfactorius).
Tamara 2014-02-15 19:22:09
Hello, I felt discomfort in my nose for about a year and now it hurts to touch my nose, what could it be?
Andrey 2013-11-05 11:58:47
Hello, I have been sick for more than 5 years, pain in the area of the lateral sinuses of the nose and frontal sinuses, it starts to hurt if the nose is blocked, then the side that is blocked is on the other side and hurts. There are no special highlights. The pain becomes stronger when I “strain my brain,” that is, when I do my homework. There is a slight curvature, but the surgeon says this is not the reason for the air not passing into the nose. It doesn’t go away, I treated it with anti-inflammatory drugs, antibiotics, physical therapy, and had a conchotomy. Also, I can’t work or study normally. Is it worth having surgery to straighten the nasal septum?
The initial section of the upper respiratory tract consists of three parts.
Three components of the nose
- external nose
- nasal cavity
- paranasal sinuses, which communicate with the nasal cavity through narrow openings
Appearance and external structure of the external nose
External nose
External nose- This is an osteochondral formation, covered with muscles and skin, in appearance resembling a hollow trihedral pyramid of irregular shape.
Nasal bones- This is the paired basis of the external nose. Attached to the nasal part of the frontal bone, they, joining each other in the middle, form the back of the external nose in its upper part.
Cartilaginous part of the nose, being a continuation bone skeleton, is firmly fused with the latter and forms the wings and the tip of the nose.
The wing of the nose, in addition to the larger cartilage, includes connective tissue formations from which the posterior sections of the nasal openings are formed. The inner sections of the nostrils are formed by the movable part of the nasal septum - the columella.
Muscular skin. The skin of the external nose has many sebaceous glands (mainly in the lower third of the external nose); a large number of hairs (in the vestibule of the nose) that perform a protective function; as well as an abundance of capillaries and nerve fibers (this explains the pain of nasal injuries). The muscles of the external nose are designed to compress the nasal openings and pull down the wings of the nose.
Nasal cavity
The entrance “gate” of the respiratory tract, through which inhaled (as well as exhaled) air passes, is the nasal cavity - the space between the anterior cranial fossa and the oral cavity.
The nasal cavity, divided by the osteochondral nasal septum into the right and left halves and communicating with the external environment through the nostrils, also has posterior openings - choanae, leading to the nasopharynx.
Each half of the nose consists of four walls. The lower wall (bottom) is the bones of the hard palate; the upper wall is a thin bone plate, similar to a sieve, through which branches of the olfactory nerve and vessels pass; the inner wall is the nasal septum; the lateral wall, formed by several bones, has the so-called nasal turbinates.
The turbinates (inferior, middle and superior) divide the right and left halves of the nasal cavity into tortuous nasal passages - upper, middle and lower. In the upper and middle nasal passages there are small openings through which the nasal cavity communicates with the paranasal sinuses. In the lower nasal passage there is an opening of the nasolacrimal canal, through which tears flow into the nasal cavity.
Three areas of the nasal cavity
- vestibule
- respiratory region
- olfactory region

Major bones and cartilages of the nose
Very often the nasal septum is curved (especially in men). This leads to difficulty breathing and, as a result, surgical intervention.
vestibule limited by the wings of the nose, its edge is lined with a 4-5 mm strip of skin, equipped with a large number of hairs.
Respiratory area- this is the space from the bottom of the nasal cavity to the lower edge of the middle turbinate, lined with a mucous membrane formed by many goblet cells that secrete mucus.
U common man the nose can distinguish about ten thousand smells, and the taster can distinguish many more.
The surface layer of the mucous membrane (epithelium) has special cilia with a flickering movement directed towards the choanae. Under the mucous membrane of the nasal turbinates lies a tissue consisting of a plexus of blood vessels, which promotes instant swelling of the mucous membrane and narrowing of the nasal passages under the influence of physical, chemical and psychogenic irritants.
Nasal mucus, which has antiseptic properties, destroys a huge number of microbes trying to enter the body. If there are a lot of microbes, the volume of mucus also increases, which leads to a runny nose.
A runny nose is the most common disease in the world, which is why it is even included in the Guinness Book of Records. On average, an adult gets a runny nose up to ten times a year, and spends a total of up to three years with a stuffy nose throughout his life.
Olfactory region(olfactory organ), colored yellowish-brown, occupies part of the upper nasal passage and the posterosuperior part of the septum; its border is the lower edge of the middle turbinate. This zone is lined with epithelium containing olfactory receptor cells.
Olfactory cells are spindle-shaped and end on the surface of the mucous membrane with olfactory vesicles equipped with cilia. The opposite end of each olfactory cell continues into a nerve fiber. Such fibers, connecting into bundles, form the olfactory nerves (I pair). Odorous substances, entering the nose along with the air, reach the olfactory receptors by diffusion through the mucus covering the sensitive cells, chemically interact with them and cause excitement in them. This excitation travels along the fibers of the olfactory nerve to the brain, where odors are distinguished.
When eating, the olfactory sensations complement the gustatory ones. With a runny nose, the sense of smell is dulled and food seems tasteless. With the help of smell, the smell of undesirable impurities in the atmosphere is detected; sometimes it is possible to distinguish poor-quality food from food that is suitable for eating by smell.
Olfactory receptors are very sensitive to odors. To excite the receptor, it is enough for only a few molecules of an odorous substance to act on it.

Structure of the nasal cavity
- Our smaller brothers - animals - are more partial to smells than humans.
- Birds, fish, and insects sense odors at great distances. Petrels, albatrosses, and fulmars are able to smell fish at a distance of 3 km or more. It has been confirmed that pigeons find their way by smell, flying for many kilometers.
- For moles, their hypersensitive sense of smell is a sure guide to underground labyrinths.
- Sharks smell blood in the water even at a concentration of 1:100,000,000.
- It is believed that the male moth has the most acute sense of smell.
- Butterflies almost never land on the first flower they come across: they sniff and circle over the flowerbed. Very rarely, butterflies are attracted to poisonous flowers. If this happens, the “victim” sits down by a puddle and drinks heavily.
Paranasal (paranasal) sinuses
Paranasal sinuses (sinusitis)- these are air cavities (paired), located in the front part of the skull around the nose and communicating with its cavity through the outlet openings (ostia).
Maxillary sinus- the largest (the volume of each sinus is about 30 cm 3) - located between the lower edge of the orbits and the dentition of the upper jaw.
On the inner wall of the sinus, bordering the nasal cavity, there is an anastomosis leading to the middle meatus of the nasal cavity. Since the hole is located almost under the “roof” of the sinus, this complicates the outflow of contents and contributes to the development of congestive inflammatory processes.
The anterior, or facial, wall of the sinus has a depression called the canine fossa. This area is usually where the sinus is opened during surgery.
The upper wall of the sinus is also the lower wall of the orbit. The bottom of the maxillary sinus comes very close to the roots of the upper back teeth, to the point that sometimes the sinus and teeth are separated only by the mucous membrane, and this can lead to sinus infection.
The maxillary sinus got its name from the English doctor Nathaniel Highmore, who first described its diseases

Diagram of the location of the paranasal sinuses
The thick posterior wall of the sinus is bordered by the cells of the ethmoidal labyrinth and the sphenoid sinus.
Frontal sinus is located in the thickness of the frontal bone and has four walls. Using a thin winding canal that opens into the anterior section of the middle meatus, the frontal sinus communicates with the nasal cavity. The inferior wall of the frontal sinus is the superior wall of the orbit. The median wall separates the left frontal sinus from the right, the posterior wall separates the frontal sinus from the frontal lobe of the brain.
Ethmoid sinus, also called the “labyrinth,” is located between the orbit and the nasal cavity and consists of individual air-bearing bony cells. There are three groups of cells: anterior and middle, opening into the middle nasal meatus, and posterior, opening into the upper nasal meatus.
Sphenoid (main) sinus lies deep in the body of the sphenoid (main) bone of the skull, divided by a septum into two separate halves, each of which has an independent exit to the area of the upper nasal passage.
At birth, a person has only two sinuses: the maxillary and the ethmoidal labyrinth. The frontal and sphenoid sinuses are absent in newborns and begin to form only from 3-4 years of age. The final development of the sinuses ends at approximately 25 years of age.
Functions of the nose and paranasal sinuses
The complex structure of the nose ensures that it successfully performs the four functions assigned to it by nature.
Olfactory function. The nose is one of the most important sense organs. With its help, a person perceives all the variety of smells around him. The loss of smell not only impoverishes the palette of sensations, but is also fraught with negative consequences. After all, some odors (for example, the smell of gas or spoiled food) signal danger.
Respiratory function- most important. It ensures the supply of oxygen to the body tissues, which is necessary for normal functioning and blood gas exchange. When nasal breathing is difficult, the course of oxidative processes in the body changes, which leads to disruption of the cardiovascular and nervous systems, disorders of the lower respiratory tract and gastrointestinal tract, increased intracranial pressure.
Plays an important role aesthetic value nose Often, while ensuring normal nasal breathing and sense of smell, the shape of the nose gives its owner significant experiences, not corresponding to his ideas of beauty. In this regard, it is necessary to resort to plastic surgeries that correct appearance external nose.
Protective function. The inhaled air, passing through the nasal cavity, is cleared of dust particles. Large dust particles are trapped by hairs that grow at the entrance to the nose; Some dust particles and bacteria, passing along with the air into the winding nasal passages, settle on the mucous membrane. Non-stop vibrations of the cilia of the ciliated epithelium remove mucus from the nasal cavity into the nasopharynx, from where it is expectorated or swallowed. Bacteria that enter the nasal cavity are largely neutralized by substances contained in nasal mucus. Cold air, passing through the narrow and winding nasal passages, is warmed and moistened by the mucous membrane, which is abundantly supplied with blood.
Resonator function. The nasal cavity and paranasal sinuses can be compared to an acoustic system: the sound, reaching their walls, is amplified. The nose and sinuses play a leading role in the pronunciation of nasal consonants. Nasal congestion causes nasal sounds, in which nasal sounds are pronounced incorrectly.














