What species of the genus corynebacterium produce exotoxin. Corynebacteria
The causative agent of diphtheria - Corynebacterium diphtheriae and a large group of microorganisms similar in morphological and biochemical properties of the genus Corynebacteria are called coryneform bacteria or diphtheroids. They are represented by gram-positive motionless rods, often with thickenings at the ends, resembling a club (coryne - a club). Diphtheroids are widely distributed in soil, air, food (milk). Among them, three ecological groups can be distinguished:
- - human and animal pathogens;
- - plant pathogens;
- - non-pathogenic corynebacteria.
Many types of diphtheroids are normal inhabitants of the skin, mucous membranes of the pharynx, nasopharynx, eyes, respiratory tract, urethra and genitals.
Diphtheria.
Diphtheria is an acute infectious disease, predominantly of childhood, which is characterized by intoxication organism diphtheria toxin and characteristic fibrinous (diphtheritic) inflammation in the place of localization of the pathogen (phther - film).
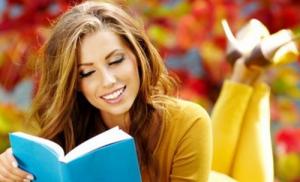
Morphological and tinctorial properties. C.diphtheriae are thin, polymorphic rods with club-shaped ends, often containing volutin inclusions, detected by methylene blue or Neisser staining. With the latter, the sticks are colored yellow - straw color, grains of volutin (polymetaphosphate) - in dark brown. In cultures, the sticks are at an angle to each other (features of division), forming various shapes - spread fingers, V, Y, L, etc. They have a microcapsule, as well as fimbriae, which facilitate adhesion to the epithelium of the mucous membranes.
Cultural properties. Diphtheria root bacteria do not grow on simple media. They require media with blood or blood serum (Leffler media, Ru), on which growth is noted after 10-12 hours, during which time the accompanying (contaminating samples) microflora does not have time to fully develop.
The most optimal Tellurite Medium and Tellurite - MacLeod Chocolate Agar. High concentrations of potassium tellurite in these media inhibit the growth of extraneous flora. Corynebacterium diphtheria reduce tellurite to metallic tellurium, which gives their colonies a dark gray or black color.
This pathogen is isolated biotypes - gravis, mitis, intermedius, differing in morphology, antigenic and biochemical properties, the severity of diseases in humans. The gravis type more often causes outbreaks and a more severe course; it is characterized by large daisy-shaped colonies with irregular edges and radial striation (R-form). Type mitis causes mainly mild sporadic diseases, forms small smooth colonies with smooth edges (S-shapes) on solid media. The intermedius type occupies an intermediate position, forms RS-forms of transitional characteristics on dense media, but even smaller ones. On liquid media, they cause turbidity of media, form a crumbly precipitate.
Biochemical properties. Corynebacterium diphtheria ferment glucose, maltose. Lack of activity in relation sucrose and urea - an important differential feature among diphtheroids. Possess cystenase activity (cleave cysteine) - Pisa test.
Antigenic structure. O- and K- antigens are isolated. Polysaccharide components of O-antigens of the cell wall have intergeneric properties, causing nonspecific cross-reactions with mycobacteria, actinomycetes (nocardia).
Surface K-antigens - capsular proteins, have species specificity and immunogenicity. There are 11 serotypes. Serotypes 1-5 and 7 belong to the gravis biovar. Serotyping of cultures is carried out in RA with diagnostic sera to the corresponding serovars and polygroup agglutinating serum.
In serological diagnostics, people often use RPHA, which is more sensitive than RA. ELISA is also currently used. Many strains of corynebacteria diphtheria (especially nontoxigenic) have spontaneous agglutinability and polyagglutinability.
Pathogenic factors. Toxigenic strains of the causative agent of diphtheria produce a strong exotoxin(thermolabile highly toxic immunogenic protein). Nontoxigenic strains do not cause disease.
The toxin causes irreversible blocking of polypeptide chain elongation, i. E. any protein synthesis. Basically, certain systems are affected: sympathetic - adrenal, heart and blood vessels, peripheral nerves. Structural and functional disorders of the myocardium, demyelination of nerve fibers, leading to paralysis and paresis are noted.
The ability to form toxin is shown only by lysogenic strains infected with a bacteriophage (beta - phage) carrying the tox gene, which encodes the structure of the toxin (i.e., carrying genes of a moderate prophage in their chromosome). Phage typing is used to differentiate strains of diphtheria corynebacteria.
Epidemiology. Reservoir - a person (sick, convalescent, bacteria carrier). The main transmission route is airborne, seasonality is autumn - winter. The pathogen is well preserved at low temperatures, dried out (saliva, mucus, dust).
Clinical and pathogenetic features. The causative agent at the site of introduction causes fibrinous inflammation with the formation of a fibrinous film tightly adhered to the tissues. The action of exotoxin (described in the section “factors of pathogenicity”) is of essential importance in the caused pathology. By localization, diphtheria of the oropharynx (most often), respiratory tract, nose and rare localization (eyes, external genital organs, skin, wound surface) is isolated. Pharyngeal diphtheria can cause croup and asphyxia.
Laboratory diagnostics. The main diagnostic method is bacteriological. Used to identify patients, carriers of bacteria, contact. Material for microscopy and cultures is taken with sterile swabs - mucus from the pharynx and nose, films from the tonsils and other places suspicious of diphtheria lesions.
The pathogen is isolated by inoculation on elective tellurite media and blood agar. On the mucous membrane of the eye, C.xerosis is often detected (a possible cause of chronic conjunctivitis), in the nasopharynx - C.pseudodiphtheriticum (Hofmann's bacillus), and other diphtheroids are also detected.
To differentiate the causative agent of diphtheria from diphtheria, indicators such as the ability to restore tellurite and form dark colonies, the Pisa test, fermentation of carbohydrates (glucose, maltose, sucrose) and urea, the ability to grow under anaerobic conditions (typical of the causative agent of diphtheria) are used.
An obligatory step is to determine the toxigenicity of the culture. The most common methods are bioassays on guinea pigs, agar precipitation reaction. ELISA with antitoxin, genetic probes and PCR are also used to detect the A fragment of the tox gene.
Treatment. Use antitoxic antidiphtheria serum, antibiotics and sulfa drugs.
Post-infectious immunity- persistent, mainly antitoxic. To quantitatively determine the level of antitoxic immunity, the Shick test (intradermal toxin injection) was previously used, now - RPHA with erythrocyte diagnosticum obtained by sensitizing erythrocytes with diphtheria toxoid.
Prevention. It is based on mass immunization of the population. Use various drugs containing diphtheria toxoid - DPT, ADS, ADS-M, AD and AD-M.
Diphtheria is considered one of the most dangerous diseases, the pathogen is called corynebacterium species (spp), a bacterium that has a rod-like shape.
The body of a healthy person contains a small amount of corynebacteria in the large intestine. With pathological changes, additional infection, the vital activity of microorganisms leads to disease.
The bacterium is divided into several types, each of which is unique, has a specific character. Based on the variety, microorganisms affect the skin, affect the work of internal organs. People with weak immunity are at risk. Bacteremia will begin to develop when bacteria infect the abdominal, venous catheters.

If men or women have corynebacteria, the likelihood of septic arthritis and pneumonia is high.
Mobileuncus
There are hidden infectious diseases including dangerous bacteria such as mobiluncus spp and corynebacterium spp present in DNA. The presence of dangerous bacteria in urine, semen or smear will lead to inflammatory processes. In men, the pathology of the urogenital tract develops, leading to orchiepididymitis, non-gonococcal and others.
Often a motile microorganism is found in female vaginal secretions, both bacterial and healthy. With accumulations of mobiluncus in the rectal area, contamination of the vagina may occur, and infection will occur during anal sex.
Several methods are used to diagnose the presence of bacteria:
- Polymerase chain reaction;
- Bacterioscopic examination.
- Serological methods.
You can become infected with the disease only through contact with a sick person. People who have previously suffered from the disease also pose a danger to others, having a pathogen bacterium in the body.

Bacteria are transmitted by airborne droplets, or they settle on household items: these are the attributes of dishes, bedding, clothes, things belonging to the category of personal hygiene, and so on. If an infected person has had contact with food, they also become the causes of infection.
People in contact with patients with acute diphtheria increase the risk of their own infection by airborne droplets.
Diphtheria is often asymptomatic for a long time, without the absence of hospitalization, the patient is able to infect many healthy people around. A recovered patient is a carrier for another 3–8 weeks, and sometimes the period increases to 3–5 months.
Treatment
To prevent corynebacteria from causing the appearance of diseases of the reproductive organs, the urinary system, before planning a pregnancy, two partners need to be tested for the presence of the bacteria.
If the tests show a positive result, doctors will prescribe a course of antibiotics. It is forbidden to self-medicate; a well-chosen treatment regimen is required for each patient.
Men living in hot and dry climates are prone to erythrasma, a pathology related to cutaneous dermatitis. The disease manifests itself in the area of bodily folds, with signs similar to dermatitis or thrush (the second name is).
When the presence of corynebacteria in a woman is diagnosed, accurate quantification is important. With moderate, a course of medication is sufficient. If the volume exceeds the norm, additional studies are performed to identify other vaginal infectious pathologies. When found, concomitant diseases are cured first.
When prescribing treatment, a woman needs to postpone conception. When at least 30 days have passed after complete recovery, you can think about pregnancy.
Question 2. Corynebacterium diphtheria Corynebacterium diphtheriae (genus Corynebacterium)
C. diphtheriae - rod-shaped bacteria; cause diphtheria (Greek diphtheria - skin, film) - an acute infection characterized by fibrinous inflammation in the pharynx, larynx, less often in other organs, and intoxication.
Morphological and cultural properties.
Corinebacterium diphteriae are thin, slightly curved or straight gram-positive rods that are angled to each other in the form of Roman fives. They are thickened at the ends due to the presence of grains valutin at one or both poles of the cell. Valatin grains consist of polyphosphates, they perceive aniline dyes more intensely than the cell cytoplasm and are easily detected when stained according to Neisser in the form of blue-black granules, while the bodies of bacteria are colored yellow-green. When stained according to Gram, the grains of valutin are not detected.

Smear drawing from pure culture. Neisser stain Pure culture smear.
Staining with Leffler's alkaline blue
Diphtheria bacillus is not acid-resistant, immobile, does not form a spore, has a microcapsule with a cord factor included in its composition. The cell wall contains galactose, mannose, arabinose, as well as a large amount of lipids, including non-acid-resistant mycolic acids.
The causative agent of diphtheria is a facultative anaerobe, heterotroph, which grows at 37 ° C on complex nutrient media: coagulated blood serum, blood tellurite agar.
On elective media, after 8-14 hours, it forms punctate, convex yellowish-cream colonies with a smooth or slightly granular surface. The colonies do not merge and look like pebbled skin.
On tellurite media, the causative agent of diphtheria forms black or black-gray colonies after 24-48 hours as a result of the reduction of tellurite to metallic tellurium.
The causative agent of diphtheria has a high enzymatic activity. Differential diagnostic signs C. diphteriae are:
lack of ability to ferment sucrose and decompose urea,
the ability to produce the enzyme cystinase.
The causative agent of diphtheria is not homogeneous in terms of cultural and biochemical properties. In accordance with the recommendations of the WHO Regional Office for Europe, C. diphteriae is subdivided into 4 biovars: gravis, mitis, intermedius, belfanti.
On tellurite medium, biovar gravis forms dry, dull, large, flat, grayish-black colonies, raised in the center. The periphery of the colony is light with a radial striation and an uneven edge. Such colonies resemble a daisy flower. Biovar mitis forms small, smooth, shiny, black, convex colonies with an even margin, surrounded by a hemolysis zone. The biovars intermedius and belfanti actually belong to the biovar mitis, since they do not decompose starch, and this trait is the most stable in C. diphteriae.
Antigenic structure. C. diphteriae have O-antigen (lipid and polysaccharide fractions located deep in the cell wall) and K-antigen (surface heat-labile protein). The O antigen is interspecies. On the basis of the K-antigen, about 58 serovars are distinguished.
Pathogenic factors. The main pathogenicity factors of C. diphteriae are surface structures, enzymes and toxins.
Surface structures (drank, microcapsule components: cord factor, K-antigen, mycolic acids) have a protein and lipid nature, promote the adhesion of microbes at the entrance gate, prevent bacterial phagocytosis, have a toxic effect on the cells of the macroorganism, and destroy mitochondria.
Enzymes of pathogenicity: neuraminidase, hyaluronidase, hemolysin, dermonecrotoxin. Neuraminidase cleaves N-acetylneuraminic acid from mucus glycoproteins and cell surfaces, lyase breaks it down into pyruvate and N-acetylmannosamine, and pyruvate stimulates the growth of bacteria. As a result of the action hyaluronidase increases the permeability of blood vessels and the release of plasma beyond their limits, which leads to edema of the surrounding tissues. Dermonecrotoxin causes cell necrosis at the site of localization of the pathogen. The plasma fibrinogen released outside the vessels comes into contact with thrombokinase of necrotic cells of the body and turns into fibrin, which is the essence of diphtheria inflammation. Inside the diphtheria film, C. diphteriae find protection from the effectors of the immune system and antibiotics, multiplying, they form in large quantities the main factor of pathogenicity -diphtheria histotoxin.
Diphtheria histotoxin has a blocking effect on protein synthesis in the organs most intensively supplied with blood: the cardiovascular system, myocardium, nervous system, kidneys and adrenal glands.
Epidemiology. Under natural conditions, only a person who does not have resistance to the pathogen and antitoxic immunity suffers from diphtheria. The disease is widespread. The largest number of patients is observed in the second half of September, October and November. The most susceptible are children of preschool and primary school age. Among adults, the high-risk group includes workers in catering and trade, schools, kindergartens and medical institutions.
C. diphteriae is resistant to environmental factors: in droplets of saliva adhering to dishes or toys, on door handles, they can last up to 15 days, on environmental objects - 5.5 months, and can multiply in milk. When boiled, C. diphteriae die within 1 min, in a 10% solution of hydrogen peroxide - after 3 min, in a 5% solution of carbolic acid and 50-60% alcohol - after 1 min.
Diphtheria histotoxin is very unstable and rapidly degrades when exposed to light, heating, and oxidation.
Pathogenesis.
Source of infection are:
1. carriers of toxigenic strains - those carriers who do not have clinical manifestations of the disease are especially dangerous, since they have antitoxic immunity.
2. Patients: Among the patients, the most important are those with the localization of the process in the upper respiratory tract. The patient is epidemiologically dangerous during the entire period of the illness, even during the recovery period, he releases toxigenic strains into the environment.
The main mechanism of infection is aerosol. Transmission ways:
the leading role belongs to airborne droplets,
sometimes air-dust, contact-household, as well as alimentary (through milk) transmission routes can be carried out.
Entrance gate infections are the mucous membranes of the oropharynx (palatine tonsils and surrounding tissues), nose, larynx, trachea, as well as mucous membranes of the eyes and genitals, damaged skin, wound or burn surface, unhealed umbilical wound.
Most common pharyngeal diphtheria ( 90-95%). The incubation period lasts from 2 to 10 days. According to the pathogenesis, diphtheria belongs to toxinemic infections when the microbe remains at the site of the entrance gate of the infection, and all clinical manifestations are associated with the action of exotoxin.
The initial stage of the infectious process is the adhesion of the microbe at the site of the entrance gate. Multiplying there, the microbe secretes g istotoxin, which has a local effect on tissue cells, and also enters the bloodstream, which leads to the onset of toxinemia.
In the area of the entrance gate, an inflammatory reaction develops, which is accompanied by necrosis of epithelial cells and edema, a white plaque is formed with a grayish or yellowish tint, containing a large number of microbes that produce toxin.
A characteristic sign of diphtheria is fibrinous film:
If the mucous membrane is formed monolayer epithelium(larynx, trachea, bronchi), occurs croupous inflammation, here the film is located superficially and is easily separated from the underlying tissues.
If the mucous membrane is formed stratified epithelium(oropharynx, epiglottis, vocal cords), occurs diphtheria inflammation, when all cells are firmly connected with each other and with the underlying connective tissue base. The fibrinous film in this case is tightly adhered to the underlying tissues and is not removed with a swab. When you try to do this, the mucous membrane bleeds.
Immunity. After the transferred disease, persistent and intense humoral antitoxic immunity is formed. The duration of post-vaccination immunity is 3-5 years.
Microbiological diagnostics.
Material for research is a fibrinous film, mucus from the throat or nose.
The collection of material must be carried out within 3-4 hours (no later than 12 hours) from the moment of the patient's visit. To take the material, dry cotton swabs are used, if the sowing is carried out within 2-3 hours, when transporting the material, the swabs are moistened with a 5% glycerin solution.
Diagnostic methods:
The main diagnostic method is bacteriological. The bacteriological laboratory should give an answer after 48 hours about the presence or absence of C. diphteriae in the analyzes.
The material is inoculated on a nutrient medium. Suspicious colonies are selected and the isolated culture is identified:
By the presence of cystinase (Pisa test): the culture under study is inoculated into a column of nutrient agar with cystine injections. Inoculations are incubated at 37 ° C for 24 hours. C. diphteriae causes blackening of the medium during the injection as a result of the formation of lead sulfide.
By the presence of urease (Sachs test): prepare an alcoholic solution of urea and an indicator solution - phenol red, which are mixed before use in a ratio of 1: 9 and poured into agglutination tubes. The bacteria under study are introduced in a loop and rubbed along the wall of the trim. In the positive case, after 20-30 minutes of incubation at 37 ° C, the medium turns red as a result of the cleavage of urea by urease.
The ability of C. diphteriae to produce toxin (established by precipitation in agar). For this, a strip of filter paper impregnated with antitoxic anti-diphtheria serum containing 5000 AU / ml is placed in a Petri dish with nutrient agar containing 15-20% horse serum, 0.3% maltose and 0.03% cystine. The dish is dried at 37 ° C for 30 minutes and the test strains are inoculated with plaques at a distance of 0.6-0.8 cm from the edge of the paper. The inoculations are incubated at 37 ° C for 24 hours. In the positive case, a precipitate in the form of white lines - "tendrils" is formed in the medium at the junction of the toxin with the antitoxin in the medium.
To determine the toxicity of the causative agent of diphtheria, it can be used bioassay. The test culture is injected into the guinea pig intradermally or subcutaneously. Toxigenic cultures kill animals within 3-5 days, autopsy reveals hyperemic adrenal glands, and with intradermal infection, skin necrosis.
For bacterioscopic examination(as an independent diagnostic method, it is rarely used due to the polymorphism of the pathogen, but it can be performed at the request of a doctor) smears are prepared from the material on several glasses, one smear is stained according to Gram, the other according to Neisser, the third is treated with fluorochrome - coriphosphine for luminescence microscopy.
The presence of antitoxic immunity is judged by the Schick reaction - the reaction of neutralizing the toxin with an antitoxin. 1/40 DLM of diphtheria toxin is injected into the skin of the forearm. Redness and swelling at the injection site indicates the absence of antitoxins in the blood. A negative Schick reaction indicates the presence of antitoxins.
For the accelerated detection of diphtheria toxin, both in bacterial cultures and in blood serum, use: RNGA with antibody erythrocyte diagnosticum, RIA and ELISA. Molecular genetic research methods are used PCR.
Preparations for the specific treatment of diphtheria.
In order to neutralize diphtheria histotoxin, use specific anti-diphtheria horse purified concentrated serum, which is obtained by hyperimmunization of horses with diphtheria antitoxin.
Specific treatment with antidiphtheria serum is initiated immediately upon clinical suspicion of diphtheria. It is necessary to choose the optimal mode of serum administration, since antitoxin can neutralize only toxin not associated with tissues. To prevent the development of anaphylactic shock, serum is administered fractionally according to A.M. Infrequently. The introduction of serum later than the 3rd day of illness is inappropriate.
Designed by human antidiphtheria immunoglobulin for intravenous administration. Its use gives fewer side reactions.
To suppress the multiplication of C. diphteriae, antibiotics must be prescribed at the entrance gate. The drugs of choice are penicillin or erythromycin, or other β-lactams and macrolides.
Preparations for the specific prophylaxis of diphtheria.
To create an artificial active antitoxic immunity, use diphtheria toxoid. The purified and concentrated preparation is included in the associated vaccines:
1.adsorbed diphtheria-tetanus pertussis vaccine (DTP vaccine),
2.adsorbed diphtheria-tetanus toxoid (ADS-toxoid),
3.adsorbed diphtheria-tetanus toxoid with reduced antigen content (ADS-M),
4. adsorbed diphtheria toxoid with reduced antigen content (AD-M).
Basic immunity is created in children according to the vaccination schedule. Only 95% coverage of the population with vaccinations guarantees the effectiveness of vaccination.
| " |
Corynebacterium group includes representatives of genera Corynebacterium represented by immobile rod-shaped bacteria capable of branching.
Corinebacteria. Corynebacterium diphtheriae
The causative agent of diphtheria. Diphtheria stick (Klebs-Loeffler stick). Diphtheria. Garotillo
Diphtheria- an acute infectious disease caused by Corynebacterium diphtheriae and its toxin. Diphtheria sticks cause inflammation of the airways, less often of the skin. Klebs-Loeffler stick toxin leads to degeneration of peripheral nerves, heart muscle and other tissues.
Diphtheria is known a long time ago; even the Syrian physician and historiographer Areteus of Cappadocia (1st century BC) described it as “malignant ulcers on the tonsils, leading to suffocation. The latter is so characteristic that in Spain diphtheria was called “ garotillo", That is, a small garota (a device used to strangle criminals).
The causative agent of diphtheria - Corynebacterium diphtheriae; it was first identified by E. Klebs(1883), and F. Loeffler (1884).
Epidemiology of diphtheria. Prevalence of diphtheria bacillus
Diphtheria reservoir- a person (sick, convalescent, bacteria carrier); the greatest epidemic danger is posed by sick persons. Reconvalescents secrete diphtheria bacillus within 15-20 days. The main route of transmission of diphtheria bacillus- airborne; infection is also possible through objects used by the sick, and contaminated food (usually milk).
At room temperature in humid atmosphere Klebs-Loeffler stick lasts a long time. At 60 ° C, diphtheria bacillus dies off within 10 minutes; in dried films it can withstand a temperature of 98 "C for 1 hour, and at room temperature it can be stored for up to 7 months.
On toys, diphtheria bacillus lasts up to 2 weeks, in dust - up to 5 weeks, in water and milk - up to 6-20 days, in diffused light it remains viable up to 8 hours. Disinfectants and antiseptics inactivate the causative agent of diphtheria within 5-10 minutes.
Peak incidence of diphtheria falls in the autumn-winter months.
1. CORINEBACTERIA
The genus Corynebacterium includes bacteria that have clavate thickenings at the ends: corynebacteria, pathogenic for humans and animals, and diphtheroids (non-pathogenic and opportunistic corynebacteria).
The causative agent of diphtheria
The discovery of the causative agent of diphtheria was preceded by extensive clinical, pathological, epidemiological and experimental studies, which largely paved the way for its detection (Klebs E., 1883), isolation in pure culture (Leffler F., 1884), obtaining toxin (Ru E. and Iersen A., 1888), antitoxic serum (Bering E., Kitazato, 1890, Roux E., 1894) and diphtheria toxoid (Ramon G., 1923).
Morphology. Diphtheria corynebacteria - Corynebacterium diphtheriae (Latin soguna mace, diphthera - film, skin) straight or slightly curved sticks 18 μm long and 03 0.8 μm wide, polymorphic, better stained at the poles on which metachromatic granules of volutin (Babesh grains Ernst, polymetaphosphates) In diphtheria corynebacteria, club-like thickenings are observed at the ends, containing volutin grains, sometimes branched and filamentous forms appear, as well as short formations, almost coccoid and yeast-like. In strokes, they are arranged in a V-shape (at an angle), taking the form of spread fingers. They do not form spores, capsules and flagella, are gram-positive.
Cultivation. The causative agent of diphtheria, aerobic or facultative anaerobic, is well cultivated on media containing protein (curdled serum, blood agar, serum agar), as well as on sugar broth. On Roux medium (coagulated horse serum) and Leffler's medium (3 parts bovine serum + 1 part sugar broth), diphtheria corynebacteria develop within 16-18 hours, their growth resembles shagreen skin, the colonies do not merge with each other.
According to the cultural and biological properties, diphtheria corynebacteria are divided into three biovars gravis, mitis and intermedius, which differ from each other in a number of ways.
Corynebacterium biovar gravis on tellurite agar containing defibrinated blood and potassium tellurite form large rough (R-shaped) rosette-like colonies of black or gray color. They ferment dextrin, starch and glycogen, form a surface film and granular sediment in broth, are usually highly toxic and have more pronounced invasive properties.
Corynebacterium biovar mitis grows on tellurium agar to form dark smooth (S-shaped) shiny colonies. They do not ferment starch and glycogen, ferment dextrin inconsistently, cause hemolysis of erythrocytes of all animal species, diffuse turbidity is noted in the broth. Cultures of this type are generally less toxigenic and less invasive than the corynebacter biovar gravis.
The corynebacterium biovar intermedius occupies an intermediate position. Their colonies on tellurite agar are small (RS-forms), black, do not ferment starch and glycogen, and grow in broth with the appearance of turbidity and granular sediment.
Enzymatic properties. Diphtheria corynebacteria (all three biovars) do not clot milk, do not decompose urea, do not emit indole, weakly form hydrogen sulfide, reduce nitrates to nitrites, as well as potassium tellurite to tellurite sulfide, as a result of which the colonies of diphtheria corynebacteria on tellurite serum agar become black or black.
Diphtheria corynebacteria ferment glucose and maltose, intermittently galactose, starch, dextrin, glycerin.
Diphtheria bacteria ferment cysteine to form hydrogen sulfide and do not decompose urea, while diphtheroid bacteria break down urea but do not ferment cysteine.
Diphtheria corynebacteria produce bacteriocins (corynecins), which endow them with some selective advantages.
Toxin formation. Diphtheria corynebacteria produce strong exotoxins in broth cultures (histotoxin, dermonecrotoxin, hemolysin). The toxicity of corynebacterium diphtheria is associated with lysogenicity (the presence of moderate prophage phages in toxigenic strains). The classic international reference strain Park Williams 8, a producer of exotoxin, is also lysogenic and retains the ability to form toxins for more than 85 years. Genetic determinants of toxigenicity (tox + genes) are localized in the genome of the prophage integrated with the nucleoid of corynebacterium diphtheria.
As a result of lysogenization, nontoxigenic strains of C. diphtheriae (biovar mitis) are converted into toxigenic ( toxigenic conversion).
Diphtheria toxin is a thermostable polypeptide consisting of two fragments called A and B. Fragment B is required to transport fragment A into the cell, where it inhibits elongation of the polypeptide chain on the ribosome. Suppression of protein synthesis is likely to provide both necrotic and neutrotoxic toxic effects of diphtheria toxin.
Diphtheria toxin is unstable. It is easily destroyed under the influence of temperature, light and atmospheric oxygen, but is relatively resistant to ultrasound.
After adding 0.3-0.4% formalin to the toxin and subsequent holding at 38 - 40 ° C for 3-4 weeks, it is converted into diphtheria toxoid, which is more resistant to physical and chemical influences than the original toxin.
Toxigenic strains of diphtheria corynebacteria, along with lysogenicity, are characterized by pronounced dehydrogenase and neuraminidase activity, while nontoxigenic strains do not have such activity.
Antigenic structure. Eleven serovars were found in the diphtheria causative agent by agglutination reaction.
The toxins formed by different strains of biovars gravis and mitis do not differ from each other and are completely neutralized by standard diphtheria antitoxin. A number of authors have established the presence of variant-specific thermolabile surface protein antigens (K-antigens) and group-specific thermostable somatic polysaccharide antigens in corynebacterium diphtheria.
Among the corynebacterium diphtheria, there are 19 phage types, with the help of which the sources of infection are identified; phage types are also taken into account when identifying isolated cultures.
Resistance. Diphtheria corynebacteria are relatively resistant to the harmful effects of environmental factors. They remain alive on rolled serum for up to 1 year, at room temperature for up to 2 months, on children's toys for up to several days. Corinebacteria persist for a long time in the films of patients with diphtheria, especially if the films are not exposed to light. From the action of a temperature of 60 ° C and a 1% solution of phenol, corynebacteria die within 10 minutes.
Pathogenicity for animals. In vivo, virulent diphtheria corynebacteria are found in horses, cows, dogs, probably infected from people who are sick and carriers. However, pets do not play a role as sources of human infection.
Of the laboratory animals, guinea pigs and rabbits are the most susceptible. When they are infected with a culture or a toxin, they develop a typical picture of toxicoinfection with the formation of inflammation, edema, and necrosis at the injection site. Internal organs are hyperemic, hemorrhages are observed in the adrenal glands. A dose of 0.06 μg of toxin kills a guinea pig weighing 250 g.
Pathogenesis of the disease in humans. The source of infection is diphtheria patients and carriers. The disease is transmitted by airborne droplets, sometimes with dust particles; transmission is also possible through various objects (toys, dishes, books, towels, handkerchiefs, etc.), food (milk, various cold dishes, etc.) infected with diphtheria corynebacteria.
Carriers play an important role in the epidemiology of diphtheria. On average, the number of carriers from convalescents and healthy individuals ranges from 3 to 5%.
The highest incidence of diphtheria is noted in the fall, which is explained by an increase in overcrowding of children at this time of the year and a decrease in the body's resistance under the influence of cooling.
Due to the presence of a diffusion factor, diphtheria corynebacteria have the ability to penetrate the blood and tissues of sick people and infected animals. Diffusion factor is an enzyme called hyaluronidase, which has the ability to break down hyaluronic acid. Factors of invasiveness include neuraminidase, necrotic factor, fibrinolysin.
In the pathogenesis of diphtheria, the leading role is played by histotoxin, which blocks protein synthesis in mammalian cells, inactivates the transferase enzyme responsible for the formation of the polypeptide chain.
In the clinic and experiment on animals, the influence on the development of the disease of pathogenic staphylococci and streptococci, which significantly increase the severity of the infection, has been proven.
In a person, at the site of the introduction of the pathogen of diphtheria (pharynx, nose, trachea, conjunctiva of the eyes, skin, vulva of the vagina, wound surface) films with a large number of diphtheria corynebacteria and other microbes are formed. The produced exotoxin causes necrosis and diphtheria inflammation of the mucous membranes or skin, being absorbed, it affects the nerve cells, heart muscle and parenchymal organs, and causes the phenomena of general severe intoxication.
Deep changes occur in the heart muscle, blood vessels, adrenal glands, as well as in the central and peripheral nervous system. Therefore, they distinguish three points of application diphtheria toxin in the body: myocardium(development of toxic diphtheria myocarditis), adrenal glands(a drop in vascular tone and blood pressure due to a decrease in the production of adrenaline), nervous system(development of paralysis and paresis).
According to the localization of the process, pharyngeal diphtheria and diphtheria croup (laryngeal diphtheria) are most often observed, followed by nasal diphtheria. Diphtheria of the eyes, ears, genitals, skin and wounds is relatively rare. Pharyngeal diphtheria accounts for more than 90% of all diseases, followed by nasal diphtheria.
Death from diphtheria of the larynx can be due to asphyxia, suffocation, because even a small diphtheria film can completely block the glottis. With pharyngeal diphtheria, most deaths are associated with heart damage due to intoxication.
Immunity... In diphtheria, immunity depends mainly on the level of antitoxin in the blood. However, it is impossible to exclude a certain role and the antibacterial complex associated with phagocytosis and the presence of opsonins, agglutinins, precipitins and complement-binding substances. Immunity in diphtheria is anti-infectious (antitoxic and antibacterial).
Shick test... The presence of anti-diphtheria antitoxic immunity can be detected using the Schick test. 1/40 Dlm of toxin for guinea pig in a volume of 0.2 ml is injected into children intradermally into the forearm. With a positive reaction, indicating the absence of antitoxic immunity, redness and swelling with a diameter of up to 2 cm appear at the injection site after 24 to 48 hours. A positive Schick reaction occurs in the absence of antitoxin or its insignificant amount in the blood serum. A negative Schick reaction is to a certain extent an indicator of immunity to diphtheria.
Due to the fact that diphtheria exotoxin causes a state of sensitization and leads to the development of severe complications in many children, the previously widely used Schick reaction is used to a limited extent.
To determine the amount of antitoxins in the blood, an indirect hemagglutination reaction with erythrocytes sensitized with diphtheria toxoid is recommended.
The most susceptible to diphtheria are children aged 1 to 4 years. In recent years, there has been a relative increase in morbidity among people 15 years of age and older.
The transfer of diphtheria leaves a weaker immunity than with other diseases of childhood (measles, whooping cough). Repeated diseases of diphtheria are observed in 6 - 7% of cases.
Treatment. Diphtheria therapy includes isolation sick, strict bed rest, early appointment antitoxin and the corresponding antibiotic therapy... Supportive therapy such as probing and ventilation may be required for airway obstruction.
Patients with diphtheria are administered antitoxic serum in doses of 5000 - 15000 ME with moderate severity of the disease and 30 000 50 000 ME for severe forms.
C. diphtheriae is sensitive to penicillin, tetracycline, rifampicin, and clindamycin. Erythromycin is preferred over penicillin for treating diphtheria of the throat, especially when treating carriers. Erythromycin- and tetrcycline-resistant strains have been described.
Antibiotic therapy has no effect on the preformed (previously formed) toxin, which quickly spreads from the site of injury and, if not neutralized with antitoxin, quickly binds to tissue cells irreversibly.
Treatment) should not wait for laboratory confirmation if there is strong clinical suspicion, since the mortality rate is directly related to the delay period before antitoxin delivery, an increase from zero to 20% between the onset of illness and day 5 of infection, the median case-fatality rate is 5- 7%.
Penicillin, tetracyclines, rifampicin, clindamycin, sulfa drugs and cardiac drugs are also used.
Antibiotics are prescribed to treat carriers. A good result is obtained by the use of tetracycline, erythromycin in combination with vitamin C.
Prevention. It consists in early diagnosis, immediate hospitalization, full disinfection of the premises and objects, identification of carriers.
Specific prophylaxis carried out by active immunization. There are several vaccines used for the specific prevention of diphtheria: 1) adsorbed diphtheria toxoid (AD-toxoid); 2) adsorbed diphtheria-tetanus toxoid (ADS-toxoid); 3) adsorbed diphtheria-tetanus pertussis vaccine (DTP vaccine). All of these drugs are used according to instructions or guidelines.
It should be noted that not all immunized children acquire resistance to diphtheria. On average, 5-10% of them remain susceptible, or refractory, i.e. unable to form antibodies after immunization. This condition is the result of immunological tolerance, agammaglobulinemia, or hypogammaglobulinemia.
Previously, diphtheria was a formidable disease in children. In Russia in 1886 - 1912. more than 250,000 people fell ill every year. The mortality rate was very high, 12-30%.
Thanks to the introduction of mandatory immunization against diphtheria, great strides have been made in the fight against this infection. The incidence of diphtheria in 1975 compared with 1913 decreased to single cases, mortality from diphtheria decreased by more than 100 times.
However, at present, diphtheria has again become an actual infection for the countries of the former USSR, including Ukraine.