Duchenne myopathy. Duchenne-Becker muscular dystrophy (mdb) Becker dystrophy symptoms
Duchenne muscular dystrophy (myopathy) is considered an extremely severe hereditary disease with a progressive course, which is characterized by primary muscle damage. This disease has been known since the middle of the nineteenth century, when the neurologist Guillaume Duchenne conducted a comprehensive analysis of muscle pathology and presented it to the scientific community. There are several variants of the course of the disease, which are separated into separate nosological forms.
Duchenne myopathy is recorded in one infant out of 4 thousand newborns. Among all classified muscular dystrophies, this form is considered the most common.
Causes
The disease is associated with a mutation in the DMD gene, which is responsible for the production of the dystrophin protein. This gene is located on the X chromosome. The main function of the dystrophin protein is to ensure the structural stability of a specific glycoprotein complex that is located on the basement membrane of the muscle cell. As a rule, the male sex suffers from Duchenne myopathy. At the same time, women can be carriers of the disease.
Clinical picture
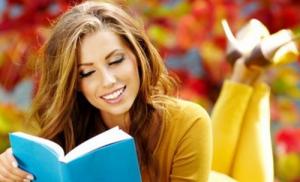
Duchenne myopathy begins to appear in boys under 5 years of age. The child is rapidly fatigued. He often falls, it is quite difficult for him to climb even stairs. What clinical symptoms will be typical:
- Progressive weakness in the legs.
- "Duck" gait. When walking, he tries to lean on the forefoot.
- Over time, muscle weakness spreads to the upper limbs, neck, torso.
- Pseudohypertrophy is revealed. The calf and deltoid muscles are increased in size due to adipose and connective tissue.
- Low stamina.
- Contractures (limitation of mobility) in the joints of the arms and legs.
- It's hard to stand without help.
- With great difficulty he gets out of bed.
- At 8-10 years of age, they can no longer walk on their own.
- Pronounced curvature of the spinal column.
- Progressive muscular dystrophy leads to the development of paralysis.
- From about 12 years of age, almost all patients cannot do without a wheelchair.
Myocardial damage is noted quite early. Children complain of shortness of breath and the appearance of painful sensations in the region of the heart. Usually death is associated with severe problems with the respiratory system and heart. The average life expectancy of patients varies from 20 to 30 years. There are isolated cases when people with muscular dystrophy lived to be 40 years old.
In most patients, serious mental abnormalities are not found, but it all depends on individual characteristics and hereditary predisposition.
Diagnostics

The characteristic clinical picture provides strong grounds for suspecting muscular dystrophy. Laboratory and instrumental diagnosis of the disease consists of the following methods:
- DNA test.
- Electromyography.
- Muscle fiber biopsy.
- Prenatal diagnostics.
Thanks to the latest technology, genetic testing can be carried out to detect mutations. In the overwhelming majority of cases, molecular genetic analysis confirms the results of other diagnostic methods. Electromyography makes it possible to assess the state of skeletal muscles and conclude that weakness is caused by damage to muscle fibers, and not by impaired nerve conduction.
If genetic testing does not reveal mutations, then a muscle fiber biopsy may be considered. In the process of this manipulation, a very small tissue sample is taken and a histological examination is performed. If the protein dystrophin is not detected in muscle tissue, it can be argued with a fairly high probability that the patient has Duchenne muscular dystrophy. It should be noted that modern DNA tests have become more accurate, and muscle fiber biopsy is used less and less.
In the case when the mother and father are carriers of a mutational gene, the risk of having a child with this hereditary pathology is very high. Whether there is a hereditary defect in the fetus - this can be determined using prenatal diagnostic methods:
- Chorionic biopsy is done at 11-14 weeks.
- Amniocentesis is acceptable after 15 weeks.
- It is possible to take blood from the fetus at 18 weeks.
When choosing one or another method of prenatal diagnosis, one should be guided by the recommendations of a geneticist. Conducting special studies in the early stages of bearing a fetus allows you to terminate a pregnancy in a timely manner in the event of a hereditary pathology. At the same time, using these diagnostic methods, the risk of miscarriage in the future increases.
The leading clinical symptom of Duchenne myopathy is progressive muscle weakness due to atrophic changes in the muscles.
Treatment

Unfortunately, to date, there is no effective treatment that will help rid the patient of hereditary Duchenne myopathy, as well as from. Considering the results of recent clinical studies, great hopes are pinned on the use of stem cells, which will have to replace abnormal muscle fibers. Nevertheless, the treatment is now symptomatic, and its main task is to try to improve the patient's quality of life. What medical methods are used:
- Symptomatic drug therapy.
- Respiratory function support.
- Use of various orthopedic aids (fixing belts, etc.).
- Physiotherapy procedures.
- Massage.
- Physiotherapy.
Despite all the efforts of modern medicine, Duchenne myopathy remains an incurable disease.
Symptomatic therapy
When using drug treatment, there is a positive trend in the course of hereditary Duchenne muscular dystrophy.
quite often used (Prednisolone, Deflazacort), which help to slow down the pathological process in muscle fibers. A therapeutic course with steroid drugs helps to increase muscle strength and reduce the severity of some clinical symptoms. However, the effect of their use persists for a short time and the risk of adverse reactions is high.
In addition, clinical studies have been conducted on the use of drugs from the beta-2-agonist group. In patients with Duchenne myopathy, they increased muscle strength but did not slow the progression of the disease. Dynamic control was carried out throughout the year. Therefore, it is difficult to talk about the long-term effect of using this group of drugs for the treatment of hereditary pathology.
Breathing support

The progression of the disease inevitably leads to serious breathing problems, as well as with. The need to use artificial ventilation is determined by the level of oxygen saturation in the blood. Currently, there is a wide selection of various portable devices that allow you to do this at home. As a rule, artificial ventilation of the lungs is already required during adolescence. But there are times when, even at the age of 20, patients do not need respiratory support.
If the breathing mask does not provide sufficient oxygenation of the blood, the following may be performed:
- Intubation (insertion of a special tube into the trachea through the nose or mouth).
- Tracheostomy operation (insertion of a tube through a tracheal incision on the front of the neck).
The duration of the use of artificial ventilation depends on the functioning of the respiratory system. If the vital capacity of the lungs falls below 30% of normal values, you should constantly use such devices. Modern types of transport artificial ventilation devices are quite compact and easy to use.
By the level of creatine phosphokinase in the blood, one can judge the degree of development and progression of Duchenne muscular dystrophy.
Stem cell therapy
Clinical research is underway to develop an effective treatment for hereditary myopathy. One of the promising areas is the use of stem cells. Scientists believe that under certain conditions these cells will be able to replace damaged muscle fibers.
In addition, gene therapy is no less promising. For example, activation of the gene responsible for the production of utrophin is of considerable interest for the treatment of hereditary Duchenne muscular dystrophy. As it turned out, this protein is, in fact, considered an analogue of dystrophin. By activating the production of utrophin, it will be possible to partially compensate for the lack of dystrophin in muscle fibers.
Physiotherapy

Each patient with Duchenne myopathy is shown physiotherapy exercises, the purpose of which is to prevent and slow down the development of contractures (limitation of mobility in the joints), as well as to improve muscle tone and strength. It is necessary to start doing exercise therapy as early as possible, immediately after the first signs of pathology appear. The level of physical activity and the set of exercises are determined individually, taking into account the severity of the disease and the general condition of the patient.
There are separate rehabilitation centers where they purposefully deal with people with this kind of disabilities. On average, 3-4 courses of exercise therapy are completed per year. In the intervals between planned physiotherapy courses, it is recommended to do physical therapy independently at home. Most parents, after preliminary instruction with a specialist, cope with this task quite well.
If the patient's condition allows and there is an opportunity, you can visit the pool. Swimming and exercise in water have a very beneficial effect on the body of a child suffering from such a serious illness. Many experts believe that in the absence of contraindications, training in the pool should be recommended to every patient with hereditary muscular dystrophy.
Lack of moderate physical activity contributes to the progression of Duchenne myopathy.
Massage
In the treatment of muscular dystrophy, special massage techniques are used. Improving muscle tone is the main task of a massage therapist. It is recommended to systematically and regularly undergo therapeutic courses. In most cases, doctors try to teach relatives about standard techniques so that at the same time they can independently perform massage at home. The positive effect is observed in patients whose treatment included a combination of physical therapy, physiotherapy procedures and massage sessions.
Physiotherapy
Complex symptomatic treatment of Duchenne myopathy almost always includes physiotherapy procedures. What effect can be expected from the use of these therapeutic methods:
- Activation of metabolic processes and improvement of trophism in muscle tissue.
- Suppression of dystrophic changes in muscles.
- Normalization of peripheral blood circulation and microcirculation.
- Improving neuromuscular conduction.
Patients with muscular dystrophy may be prescribed the following physical treatments:
- Electrophoresis.
- Laser therapy.
- Hydromassage.
- Balneotherapy.
- Infrared irradiation.
- Phonophoresis.
Forecast
In Duchenne myopathy, the pathological process extends to all types of muscles: skeletal muscles, myocardium, bronchial smooth muscles, etc. Usually, the average life expectancy does not exceed 30 years. In isolated cases, patients with hereditary muscular dystrophy can survive to the age of 40. Correct organization of patient care and the use of all modern means that can alleviate his condition can increase life expectancy.
The main method of disease prevention is prenatal diagnosis. Having identified a serious hereditary pathology in the early stages of bearing a fetus, you can make a timely termination of pregnancy.
) is one of the most common neuromuscular diseases. It is caused by mutations in the dystrophin gene. Dystrophin is found in large quantities in the area of the sarcolemma, maintaining the integrity of the muscle cell membrane. Structural changes in the sarcolemma lead to degeneration of cytoplasmic components, increased entry of potassium ions into the fibers, which causes the death of myofibrils.
It is inherited in a recessive pattern linked to the X chromosome.
Clinically separated two diseases - Duchenne muscular dystrophy and Becker muscular dystrophy - are genetically a single form of Duchenne / Becker muscular dystrophy
Duchenne myodystrophy occurs with a frequency of 3 in 10,000 newborn boys. The disease usually manifests itself at the age of 3-5 years with progressive muscle weakness. Boys often fall, lag behind their peers in games, run and jump with difficulty. By the age of 5, muscle weakness is revealed on examination. From a sitting position on the floor, the patient gets up, leaning first on his own knees, then on his hips (a symptom of a ladder). As a rule, the legs are thickened, and the true hypertrophy of the gastrocnemius muscles at the onset of the disease is replaced with pseudohypertrophy over time - the muscle is replaced by adipose and connective tissue. Often there are pseudohypertrophies of the deltoid, gluteal, abdominal muscles, and tongue. By the age of 6, contractures of the Achilles tendons and the iliotibial tracts are formed, the gait is noticeably changed - on tiptoes, with hyperextension in the lumbar spine ("duck" gait). The process of muscle atrophy gradually acquires an ascending direction: thigh muscles - pelvic girdle - shoulder girdle - arms. Children develop lumbar lordosis, pterygoid scapula. Muscle weakness increases, mainly the proximal muscles of the legs (especially) and arms, neck flexors are affected. Later, usually after several years, immobility develops, joint contractures (due to a predominantly sitting position) and movement in the hip, knee, elbow, wrist joints is limited .. From 8-10 years old, patients need crutches, By the age of 12, patients are chained to a wheelchair ... Contractures become irreversible, scoliosis often occurs and progresses, causing pain. This deforms the chest and worsens lung function, which already suffers from muscle weakness. At the age of 16-18, severe pneumonia often develops, often with a fatal outcome. Other causes of death are aspiration of food and acute expansion of the stomach. The atrophic process also develops in the heart (cardiomyopathy). Acute heart failure is the cause of death. The motility of the gastrointestinal tract is impaired. In the very last stage, muscle atrophy invades the muscles of the face, pharynx and respiratory muscles. Patients die in the 2-3rd decade.
Becker's myodystrophy is a benign form. The incidence in newborn boys is 3: 100,000 (10 times less common than Duchenne myodystrophy). The onset of the disease is not earlier than 10-15 years, the course is mild, patients remain functional at the age of 20-30 years. Intellectual disabilities and cardiomyopathy are not noted.
Although almost all patients have heart disease, it is rarely the cause of death. Heart failure occurs only with severe concomitant diseases, such as pneumonia.
Duchenne muscular dystrophy is a severe X-linked disease, for which there is still no effective treatment. In one of the last numbers Science as many as three articles have been published on the successful testing of CRISPR / Cas9 technology in mouse models for the treatment of this disease. Maybe this approach has a chance to get to clinics as well?
Dystrophin is located on the intracellular surface of the sarcolemma along the entire length of muscle fibers and is part of the dystrophin-associated glycoprotein complex (DAGC, DGC). It binds at one end to the F-actin of the cytoskeleton, and at the other end to β-dystroglycan, which stabilizes the fibers during contraction. The dystrophin gene is one of the longest in humans.
Figure 1. Mutations in dystrophin - the cause of the development of Duchenne muscular dystrophy. a - Dystrophin binds to actin filaments (part of the cytoskeleton) through the N-ABD and ABD2 domains) and to DAGA through the CR and CT domains. b - The crystal structure of dystrophin N-ABD. The actin binding zones are shown yellow, four well-studied disease-causing mutations - red.
They still do not know how to cure Duchenne muscular dystrophy, and today's therapy is aimed at slowing the progression of the disease and treating complications. The "gold standard" is corticosteroids, which were proposed as a treatment several decades ago. However, their use has many side effects.
It is not surprising that many groups of geneticists and molecular scientists are developing pre- and postnatal treatments for Duchenne muscular dystrophy. The disease is mainly studied in various strains of mice. In one of the last numbers Science published three independent papers at once on the treatment of Duchenne muscular dystrophy. The research teams were led by Eric Olson ( Eric Olson) from the University of Texas, Amy Wadgers ( Amy wagers) from Harvard University and Charles Gersbach ( Charles gersbach) from Duke University. All groups used the exon skipping technique to restore muscle function, in which one or more exons are removed from the mRNA (Fig. 2). In this case, the protein turns out to be shorter, but it can still perform its supporting and anchoring functions in the muscle fiber, and the "annoying circumstance" - the extra stop codon - also turns out to be "missed".

Figure 2. Exon skipping in the dystrophin gene in Duchenne muscular dystrophy. a - In patients with DMD in the gene DMD there are mutations that disrupt the reading frame during protein synthesis. For example, when exon 50 is deleted, "extra-frame" mRNA appears, which leads to the synthesis of truncated non-functional or unstable dystrophin (left)... In one of the therapeutic approaches, the antisense oligonucleotide "masks" exon 51, and it is "skipped" during splicing, the reading frame is restored. The result is a shorter but partially functional dystrophin (on right)... In new works, “extra” exons are simply excised from the genome using CRISPR / Cas9. b - Multi-exone skip in DMD therapy. If exons 45–55 are skipped, mutations of which occur in approximately 63% of patients, the resulting short dystrophin will lead to the transformation of the standard DMD phenotype into an asymptomatic or milder BMD phenotype.
The exon deletion strategy even has advantages over recreating the full length of the gene: it is easier to develop than to restore the individual deletions of each patient.
To cut out "extra" nucleotide sequences, the researchers used the technology of genome editing CRISPR (clustered regularly interspaced short palindromic repeats) / Cas9 (CRISPR-associated protein 9), which, by the way, was just allowed to be used in experiments on embryos by a London institute.
You can read more about this technique, borrowed from bacteria, in the articles: “ CRISPR systems: immunization of prokaryotes», « Mutagenic chain reaction: genome editing on the brink of fiction" and " Should we not aim at ... changing the genome?» .
Competing labs: who will be the first to translate technology into human therapy?
Scientists from three laboratories successfully apply exon skipping technology in vivo on a standard object - mice - and showed that their method helps to restore the reading frame and partially restore dystrophin synthesis. Since even a low level of it (3-15% of normal) brings therapeutic benefits, the results of the work can be called successful.
This is not the first time Eric Olson's group has used the CRISPR / Cas9 method in their work on Duchenne muscular dystrophy. In 2014, scientists corrected a mutation in the germ line of mice and prevented the development of the disease. However, since prenatal editing of the genome in human embryos is (yet?) Prohibited, researchers had to come up with a way to apply the technology postnatally.
In their last work, adeno-associated virus-9 (AAV9, adeno-associated virus-9) was used to deliver the components necessary for editing into the tissue. The researchers tested several methods of administering AAV9 on different days after birth of the mice. In all cases, the expression of the dystrophin gene in the cardiac and skeletal muscles was restored, but to a different extent. Moreover, protein production increased from 3 to 12 weeks post-injection, and skeletal muscle function improved 4 weeks post-injection. "The challenge now for Wellstone researchers is to translate the findings from the mouse model to patients with muscular dystrophy." says Pradeep Mammen, co-director of the Wellstone Center.
Amy Wagers' group conducted a similar experiment in many ways. After many preparatory stages of work on genome editing and exon skipping in cells and animals, their experience was also crowned with success: programmable CRISPR complexes in the composition of adeno-associated virus (AAV) were delivered by local and systemic administration to differentiated skeletal fibers, cardiomyocytes and satellite muscle cells newborn and adult mice. If the editing is directed only to muscle fibers, then the effect may fade over time. However, as Wadgers notes, editing genes in satellite cells can provide much longer lasting results. It can lead to the creation of a pool of regenerative cells carrying the edited dystrophin gene, and as a result of normal muscle repair, the edited gene will also be found in muscle fibers.
Finally, as everyone has already guessed, scientists led by Charles Gersbach also discovered the therapeutic effect of using AAV-CRISPR / Cas9 in a mouse model. Intraperitoneal administration of the viral vector to newborn mice resulted in the restoration of dystrophin synthesis in the abdominal muscles (muscles of the abdomen), diaphragm and heart seven weeks after injection. As the authors note, therapy of the heart and lung muscles is extremely important, since it is their refusal that often leads to the death of patients with Duchenne disease. Intravenous administration of AAV vectors to six-week-old mice also resulted in a significant restoration of dystrophin production in the heart muscle. “There is still a lot of work to be done to convert [technology] into human therapy and confirm its safety., says Gersbach. - But the results of our first experiments are already very encouraging. "... The group intends to optimize the delivery system and evaluate the effectiveness and safety of the strategy in larger animals (Figure 3). Which of the three laboratories will overtake the others and be the first to conduct human testing?
Duchenne muscular dystrophy therapy: old and new approaches
Other studies show that restoration of the normal level of synthesis of nitric oxide (NO), which decreases in patients due to impaired activity of NO-synthase (nNOS), reduces inflammation, increases the activity of its own stem cells and reconstructs the morphology and function of skeletal muscles.
The drug Givinostat is already in phase II clinical trials - histone deacetylase inhibitor that slows the progression of the disease in a mouse model.
Such a massive experimental blow to Duchenne muscular dystrophy gives hope. Will CRISPR / Cas9 technology lead the way in developing therapies that clinicians can adopt? Perhaps not far off the publication of similar works on other diseases, where you need to get rid of mutations in a single gene? We will learn this from the next issues. Science(as well as other honorary magazines).
Literature
- van Putten M., Hulsker M., Nadarajah V. D., van Heiningen S. H., van Huizen E., van Iterson M. et al. (2012). The effects of low levels of dystrophin on mouse muscle function and pathology. PLoS One. 7 , e31937;
- Russo F.B., Cugola F.R., Fernandes I.R., Pignatari G.C., Beltrão-Braga P.C. (2015). Induced pluripotent stem cells for modeling neurological disorders. World J. Transplant. 5 , 209–221;
- Falzarano M.S., Scotton C., Passarelli C., Ferlini A. (2015). Duchenne muscular dystrophy: from diagnosis to therapy. Molecules. 20 , 18168–18184;
- Bushby K., Finkel R., Birnkrant D. J., Case L. E., Clemens P. R., Cripe L. et al. (2010).
WHAT IS MUSCULAR DUSHENN / BECKER DYSTROPHY?
Muscular dystrophies Are genetic diseases characterized by progressive muscle wasting and weakness, beginning with microscopic changes in them. As the muscles break down, their strength decreases.
In the early stages of DMD and BMD, muscles in the chest (the shifting shoulders), trunk, and upper and lower leg muscles are affected. Weakness in these muscles makes it difficult to stand up, climb stairs, and maintain balance.
Duchenne muscular dystrophy (DMD) was first described in 1860 by the French neurologist Guillaume Benjamin Amand Duchenne. (MDB) is named after the German doctor Peter Emil Becker, who described this variant of MDD in 1950.
With DMD, signs of muscle weakness usually appear in boys around the age of 3 years. The disease gradually weakens the skeletal or voluntary muscles of the arms, legs, and trunk. Around early adolescence, or even earlier, the heart and respiratory muscles may also be affected.
MDB is a milder form of MDD. It usually begins in adolescence or early adolescence, and is slower and much less predictable than DMD.
(Although DMD and BMD occur almost exclusively in boys, in rare cases, girls can also be affected. "Is this family?")
WHAT CAUSES DUSHENN AND BECKER MUSCLE DYSTROPHIES?
Until 1980, very little was known about the causes of any type of muscular dystrophy. In 1986, researchers identified a gene in which defects, called mutations, caused DMD. In 1987, an associated protein was identified and named dystrophin.
Genes contain codes, or recipes, for proteins (proteins), which are very important biological components of all life forms. DMD develops when a specific gene located on the X chromosome loses its ability to make the protein dystrophin. BMD is caused by slightly different mutations in the same gene. People with BMD have some amount of dystrophin, but it is either insufficient or impaired. The presence of some dystrophin in BMD protects the muscles from degeneration as severe and rapid as in DMD.
Muscles are made up of bundles of fibers (cells). A group of independent proteins located along the membrane surrounding each fiber help muscle cells to function properly.
When one of these proteins, dystrophin, is absent, it causes Duchenne muscular dystrophy, if it is not enough or is defective, Becker muscular dystrophy develops.
Incidentally, eating or not eating foods rich in protein cannot replace lost dystrophin. For more information on how a gene mutation leads to the development of Duchenne and Becker dystrophies, see. "Is this family?"
WHAT HAPPENS TO THE MUSCLES OF PEOPLE WITH DUSHENN AND BECKER DYSTROPHIES?
Duchenne myodystrophy
The development of DMD is fairly predictable. with this disease they often start walking late. During this period, an increase in the calf muscles, or hypertrophy, may be noticed. During preschool years, children with DMD can look awkward and fall frequently. You soon have trouble climbing stairs, getting up from the floor, or running.
At school age, children may begin walking on their toes or toes with a slightly rolling gait. The gait becomes waddling and unsteady, and they can easily stumble and fall. Trying to maintain balance, they bulge their belly and throw back their shoulders. Difficulty raising arms also occurs.
Nearly all children with DMD lose their ability to walk between the ages of 7 and 12. In adolescence, assistance or mechanical aids are required to keep the arms, legs, and trunk active.
Becker's myodystrophy
Often, the diagnosis of Becker muscular dystrophy cannot be made until adolescence or even early adolescence, for example, when young people notice that they have difficulty in physical education or military training. Trying to compensate for muscle weakness, boys begin to walk with a waddling gait, on their toes or fingertips, protruding their abdomen.
As with DMD, muscle wasting in BMD usually begins in the hip, pelvic, hips, and shoulders. However, in BMD, the degree of muscle degeneration varies widely from person to person. Some require a wheelchair by the age of 30 or a little later, while others make do with minimal tools such as a cane for many years.
WHAT TESTS ARE USED TO DIAGNOSE DMD / BMD?
In diagnosing any form of muscular dystrophy, the doctor usually begins by familiarizing himself with the patient and family history and performing a physical examination. Quite a lot can be gleaned from this, including the nature of the weakness. History and examination begins a long journey towards the upcoming diagnosis even before any more complex diagnostic tests are performed.
Because the muscles in the legs are weakened, boys with DMD use a characteristic method of standing up from the floor called the Govers technique. First, they lean on their hands and knees, then raise their pelvis, and then "step" with their hands up the legs to lift the whole body.
It is important to get a correct diagnosis, as other diseases have some of the same symptoms as DMD / B. BMD can often be undetected or misdiagnosed as end-girdle muscular dystrophy (CPMD) or spinal muscular atrophy (SMA). For this reason, it is important to conduct both genetic testing and muscle biopsy before deciding whether it is BMD.
The doctor also wants to determine if the muscle weakness is caused by problems in the muscles themselves, or in the nerves that control those muscles. The nerves that control muscles, or motoneurons that radiate from the spinal cord and brain and extend to all muscles, can cause muscle weakness similar to that caused by muscle problems, although they are really different things.
Usually, the nature of the weakness can be clarified with a physical examination. Sometimes a special test called an electromyography or nerve conduction test is done. This test measures the electrical activity of the muscles and stimulates the nerves to see if the problem lies in the muscles or nerves.
At an early stage of diagnosis, doctors often prescribe a blood test to determine the level of CPK. CPK stands for creatine phosphokinase, an enzyme leaked from damaged muscles. When the level of CPK in the blood is high, it usually means that the muscles are being destroyed as a result of some pathological process, such as muscular dystrophy or inflammation. Consequently, a high level of CPK suggests that muscle weakness is caused by pathological processes in the muscles themselves, but cannot indicate exactly what kind of muscle disease this may be.
To determine which disease is causing the problem, your doctor may order a muscle biopsy, the surgical removal of a small piece of muscle from a patient. By examining this sample, the doctor can tell a lot about what actually happens to the muscles. Modern techniques make it possible, on the basis of a biopsy, to distinguish muscular dystrophies from inflammatory and other diseases, as well as to distinguish various forms of dystrophies.
Other tests using biopsies can provide information about which protein is present in muscle cells, and whether it is present in normal amounts and in its place. This can help distinguish between DMD (no dystrophin) and BMD (some amount of defective dystrophin). MR (magnetic resonance) may also be prescribed. This painless scan allows the doctor to visually determine what is going on inside the weakened muscle.
The availability of DNA diagnostic tests that use either blood cells or muscle cells to provide accurate genetic information is rapidly evolving. You can check with your doctor or genetic counselor which tests are available. Since many men with BMD (and some with DMD) become fathers, it is important to know exactly what kind of inherited disorder a person has. Sisters of people with DMD or BMD may also be tested to find out if they are carriers of the disease, as they may have children with the disease.
IS THIS FAMILY?
Upon learning that a child has a genetic disorder, such as DMD or BMD, embarrassed parents often ask: "But this was not in our family, how could it be genetic?"
DMD can be common in a family, even if only one family member has it. This is due to the inheritance mechanism of genetic diseases.
Both MDD and MDB are inherited in the so-called X-linked pattern. This means that the gene, the mutation in which causes the disease, is located on the X chromosome.
Every male child receives an X chromosome from his mother, and a Y chromosome from his father, which makes him a boy. Female children receive two X chromosomes, one from each parent.
Every son born to a woman with a mutation in the dystrophin gene on one of her two X chromosomes has a 50% chance of inheriting the damaged gene and having DMD or BMD. Each daughter of such a woman has a 50% chance of inheriting the mutation and becoming a carrier. Carriers usually have no symptoms of the disease, but they may have children with the mutation or the disease.
So how is it that a family that has not had a history of DMD or BMD suddenly has a son with this condition?
There can be two explanations for this:
A genetic mutation that leads to the development of DMD or BMD can be present in women for generations without anyone knowing about it. Boys with the disease may not have been born, or, even if the boy was sick in the early generations, relatives might not know what the disease was.
Another explanation is that a child with DMD or BMD has a new genetic mutation that has arisen during fetal development. As soon as someone develops a genetic disease, even if the mutation is spontaneous (new) in this person, he can pass it on to his offspring.
Men with DMD or BMD cannot pass on the damaged gene to their sons, because they pass on the Y chromosome, not the X. But they can certainly pass it on to their daughters, since each daughter receives only the X chromosome from the father. They will be carriers, and each of their sons will have a 50% chance of having the disease, and so on.
WOMEN AND DMD
Why don't girls have DMD or BMD? When a girl inherits a damaged gene from her mother, she usually also receives a “healthy” dystrophin gene from her father, which makes enough protein to prevent the development of the disease. Boys who inherit the mutant gene are sick because they lack a second dystrophin gene to compensate for the damage to the first.
However, although girls usually do not develop full DMD or BMD, some women who carry the damaged gene are still somewhat ill. A small percentage of female carriers are so-called "pronounced carriers", and the disease manifests itself in them in a mild form.
In such women, dystrophin deficiency can manifest as weakness of the muscles of the back, arms and legs and their rapid fatigability. Expressed carriers also have heart problems, which may present with shortness of breath or inability to do simple exercise. Heart problems, if left untreated, can be quite serious and even life-threatening.
All women who are potential carriers of DMD / BMD would be wise to undergo a full diagnostic screening to ascertain their status. Later, if carriage is confirmed, regular strength assessments and heart monitoring can help manage symptoms that are prone to worsening.
WHAT CAN BE DONE TO TREAT DMD / MBD?
Thanks to advances in many fields of medicine, there are very good therapeutic methods that can help with all manifestations of Duchenne and Becker muscular dystrophies. These methods of influence are constantly being improved. Using all available methods, patients can prolong their vigor, activity and life expectancy.
Contractures
The impact of the disease can be substantially minimized by keeping the body as flexible, straight and mobile as possible. There are several ways to accomplish this.
As muscles break down, people with muscular dystrophy often develop stiff joints called contractures. If left untreated, they will become quite severe, causing discomfort and limiting mobility and flexibility. Contractures can affect the knees, hips, feet, elbows, wrists, and fingers.
However, there are many ways to minimize and delay contractures. Range-of-motion exercises, performed regularly, can help slow contractures by preventing tendons from shortening prematurely. It is very important that a physical therapist shows you how to do these exercises correctly.
Splints on the arms and legs can also help keep the limbs stretched and mobile, delaying the onset of contractures.
When contractures develop, surgery can help to loosen them. A tendon lengthening procedure called Achilles tendon surgery is often done to treat ankle contractures while the baby is still walking. The child usually needs to use splints on his feet afterwards.
Curvature of the spine
In adolescents with DMD, the spine may gradually take on a curved shape. This curvature can occur from side to side (scoliosis), or longitudinally to form a hump (kyphosis). Occasionally, those who are still walking have a concave curvature in the lumbar spine called lordosis.
Severe scoliosis can interfere with sitting, sleeping and even breathing and should therefore be avoided.
You can consult a physiotherapist about what exercises are necessary to keep your back as straight as possible, as well as about the correct positions during sitting and sleeping.
The surgical method to correct the curvature is to insert metal rods into the spine. Usually such operations are performed at the age of 11-13 years.
Medicines
Medications are a group of drugs known as corticosteroids that have been shown to be effective in slowing the progression of DMD (there is insufficient evidence for or against corticosteroids in BMD)
In 2005, the American Academy of Neurology published guidelines for the use of these drugs for DMD. They are as follows:
Prednisolone or deflazacort has an effect in the treatment of DMD. Seven years of research has shown that their use increases strength and improves muscle timing (such as time spent climbing stairs) and lung function.
Effective starting doses: 0.75 mg per kg of body weight daily for prednisone, and 0.9 mg per kg of body weight for deflazacort
The dose should be reduced if there are serious side effects such as significant weight gain, thinning of the bones (osteoporosis), or behavioral problems. The most common side effects are weight gain and a round, puffy face
It is not yet clear that deflazacort has fewer side effects than prednisone
The optimal age for initiation of corticosteroid therapy has not been determined. Some doctors are convinced that it should be started immediately after the diagnosis is made, while others prefer to wait for the time when the boys have the first problems with walking. The physician should discuss the expected positive and potential side effects with the parent before starting corticosteroid therapy.
Calcium supplements and vitamin D are often given in combination with prednisone to neutralize its unwanted effects on bones
Drugs are sometimes prescribed for DMD or BMD to reduce the burden on the heart (see section 4.4). "How else do DMD and BMD affect the body?")
Clamps, verticalizers and wheelchairs
Braces, also called orthoses, support the shin and foot, or wrap around the knee.
Ankle braces are sometimes prescribed for use at night to prevent the baby's foot from drooping while sleeping
Standing for some time during the day, even with minimal weight bearing, promotes better circulation, strengthens bones, and straightens the spine. Walkers or verticalizers can help people with DMD and BMD in this. Some wheelchairs also have an upright position
Sooner or later, all boys with DMD need a wheelchair. Many people first use wheelchairs at school or for a walk while continuing to walk at home. With DMD, the need for constant use of the wheelchair usually occurs at the age of about 12 years. Although many children and their parents perceive wheelchairs as a symbol of disability, most believe that using them allows them to be more mobile, active and independent than trying to walk at all costs on very weak legs.
Other devices can help those caring for people with DMD or BMD. Among the simplest are transfer platforms for assistance in transferring from a stroller or a stroller. You can also use mechanical (more often hydraulic) lifts, folding chairs and electronically controlled beds.
HOW STILL DO DMD AND CSBM IMPACT THE BODY?
Pain and sensitivity
You can rest easy knowing that muscle wasting in DMD and BMD is usually painless on its own. Some people talk about recurring muscle cramps, which are usually relieved by over-the-counter pain relievers
Also, because muscular dystrophy does not directly affect nerves, people with muscular dystrophy maintain normal touch and other senses. They also tend to control the smooth, or involuntary, muscles of the bladder and intestines, and maintain normal sexual function.
Heart
Similar to the muscles of the limbs, the heart muscle can also be weakened due to a lack of dystrophin. Over time, sometimes before the age of 10 years, the cardiac problems associated with DMD can become life-threatening. Thus, careful monitoring of the cardiovascular system is necessary, usually carried out by a pediatric cardiologist.
Dystrophin deficiency often causes heart muscle weakness in people with DMD and BMD. The muscle layer of the heart (myocardium) degenerates in the same way as skeletal muscle, which can lead to fatal cardiac problems
Some people with BMD have less severe skeletal muscle damage but have serious cardiac problems
In 2005, the American Academy of Pediatrics formulated guidelines for people with DMD and BMD, as well as those with these conditions.
For patients with DMD, it is recommended to undergo a complete cardiac examination in early childhood, and then every 2 years until the age of 10 years. Further testing should be done every year, or if symptoms of heart failure such as fluid retention and shortness of breath appear.
Carriers of DMD and BMD have a higher than average risk of developing cardiomyopathy. Experts believe that carriers should undergo a complete cardiac examination in late adolescence or early adulthood, or rather - when symptoms appear, and thereafter - to undergo such examinations every 5 years, starting at 25-30 years of age.
There is preliminary evidence that treatment with angiotensin-converting enzymes (ACE) and beta-blockers can slow the damage to the heart muscle in DMD and BMD if treatment is started as soon as echocardiogram (ultrasound of the heart) is found to have abnormalities, without waiting for symptoms to appear.
Some patients with BMD with serious cardiac problems and good general condition have been successfully treated with heart transplantation.
Respiratory function
When boys with DMD reach about 10 years of age, the diaphragm and other muscles that control the lungs weaken and the lungs are less efficient at performing their function. Problems that signal insufficient respiratory function are headaches, decreased mental activity, difficulty concentrating or staying awake, and nightmares.
People with a weakened respiratory system are also more prone to infections and have difficulty coughing. Simple hypothermia can lead to the development of pneumonia. When an infection develops, it is very important to get immediate medical attention in order to prevent severe respiratory failure.
When respiratory function is impaired, one may purchase a ventilator or learn procedures to help cough up and keep the bronchi free of secretions. You can get the necessary information from a therapist or pulmonologist
In some cases, forced ventilation may be required to ensure adequate movement of air into and out of the lungs. Sometimes a breathing mask is only required at night. If necessary more often, a tracheotomy may be performed (a tube is inserted directly into the trachea to provide air to the lungs)
There are effective non-invasive ventilation systems to avoid the use of tubes. Even for those who have tubes installed in their trachea, it is sometimes possible to disconnect them from the apparatus for a while during the day. More modern tubes have valves in their design that allow speaking.
Intellectual ability
About a third of boys with DMD have some degree of cognitive lag, and some have severe cognitive lag. Experts believe that a dystrophin deficiency in the brain can cause cognitive and behavioral abnormalities. The learning problems seen in some people with DMD and BMD manifest themselves in three main areas: focusing, verbal learning and memory, and emotional interaction.
If there is a suspicion that the child has some mental retardation, it is necessary to contact a pediatric neuropsychologist. If this is confirmed, educational and psychological interventions should be initiated immediately. The professional can recommend exercises and other ways to interact with the child that will help him make up for this deficiency.
CAN SPECIAL DIETS OR EXERCISE HELP FOR DMD AND BMD?
Diet
Many people, hearing the words "protein loss", logically ask the question: "Do I need to consume more protein?" Unfortunately, eating a diet high in protein has no effect on proteins missing in muscular dystrophy.
No special dietary restrictions or supplements are known to help with DMD or BMD. The combination of inactivity and weakness in the abdominal muscles can cause severe constipation, so the diet should be high in fluids and fiber, with a predominance of fresh fruits and vegetables.
Boys who use electric wheelchairs, take prednisone, and who are not overly active may need to restrict their calorie intake to maintain their weight. Obesity puts additional strain on already weakened muscles and heart. Experts believe that a low-calorie diet does not have any harmful effects on muscles.
A low sodium diet may also be needed for those on prednisone who have heart problems.
Exercises
Exercise can help build muscle, maintain a healthy cardiovascular system, and promote wellness. However, with muscular dystrophy, excessive exercise can damage the muscles. Talk to your doctor about the best physical activity. With DMD and BMD, moderate exercise is possible, but not to the point of exhaustion.
The supportive ability of water can help prevent some types of muscle tension and damage. Before starting any exercise program, you must have a cardiac examination.
Physical and occupational therapy
Physiotherapy is usually part of a combination therapy for DMD and BMD. A physical therapist should be consulted to assess the physical condition and develop a physiotherapy program. The main goals of physiotherapy are to maintain joint mobility, prevent contractures and scoliosis.
Occupational therapy is more focused on specific activities and functions, as opposed to physical therapy, which focuses on mobility and, where possible, strengthening large muscle groups.
Occupational therapy can help with tasks related to work, play and daily life, such as getting around, dressing, or using the computer.
HOW TO LIVE WITH IT?
When a family member has DMD or BMD, the whole family has a need for support and emotional responses. Many seek help and support from religious sources, communication with families with similar experiences, psychology books, or consultations with specialists. These experts usually recommend the following:
For kids
Answer children's questions about the disease as they grow up honestly and in an accessible language
Always present the child as a person, with the disease as only one aspect of his life.
Emphasize what the child can do and help him do what he wants. Children often find ways to play sports or other hobbies
Raise him like any other child with patience, responsibility, hope and love. Avoid overprotectiveness and help him become independent.
Do normal family activities, including vacations and entertainment. With imagination and patience, you can find ways to do almost anything.
For family
Be attentive to each other's emotions and stress levels, be patient and kind
Plan regular breaks from caring responsibilities
Deal with illness problems as they arise. Don't focus on future complications
Give yourself credit for the effort and difficulty of your responsibilities
Organize a support team and ask for help when needed
Research to find treatments for DMD
Since 1986, when the gene in which mutations cause DMD and BMD was identified, scientists have made great strides in understanding the mechanisms of these diseases. Several avenues are currently being developed to find ways to stop or reverse muscle breakdown in these conditions.
Some researchers have created a working dystrophin gene without mutations, and are currently testing its safety in a small clinical study in boys with DMD.
Other researchers are testing PTC124, a drug that alters the way cells read genetic information. In about 15% of patients with DMD, the molecular stop signal is positioned too early for complete dystrophin to be synthesized. PTC124 causes cells to ignore this signal
More researchers are experimenting with antisense nucleotides, compounds designed to induce cells to bypass certain types of genetic errors, not just stop signals. These formulations have passed laboratory tests and the first clinical trials have shown promising results.
Other research groups are using stem cells from muscle, blood vessels, or bone marrow to try to regenerate muscle
Finally, several groups are developing strategies to enhance protein synthesis atrophin, which is very similar to dystrophin but is synthesized in people with DMD and BMD. Experiments show that increasing atrophin levels can compensate for dystrophin deficiency to some extent.
A summary of the main studies can be read
Duchenne myodystrophy (DMD)- hereditary disease that begins at the age of 2-5 years and is characterized by progressive muscular weakness, atrophy and pseudohypertrophy proximal muscle, often accompanied by cardiomyopathies and intellectual impairment. In the early stages of the disease, there is increased fatigue when walking, a change in gait ("duck gait"). In this case, there is a gradual degradation of muscle tissue. 95% of patients stop walking at the age of 8-12 years. At the age of 18-20, patients usually die, often from respiratory failure. An allelic form of DMD is distinguished - Becker's muscular dystrophy (BMD, OMIM), which is characterized by similar clinical manifestations, a later onset (at about 10-16 years of age) and a milder course. Such patients often retain the ability to walk for up to 20 years, and some up to 50-60 years, although the same muscles are involved in the pathological process as in DMD. The life expectancy of such patients is reduced slightly.
A biochemical marker of the disease is an increased (100-200) times the level of creatine phosphokinase (KFK) in blood. In carriers of the damaged gene, the CPK level is also slightly increased on average.
The type of inheritance of Duchenne muscular dystrophy is X-linked recessive, i.e. it affects almost exclusively boys, while women with a damaged gene on one of the X chromosomes are carriers of DMD. But in rare cases, girls can also be ill with Duchenne muscular dystrophy. The reasons for this may be the predominant inactivation of the X chromosome with a normal allele in heterozygous carriers of the mutant DMD gene, X autosomal translocation affecting this gene, hemizygosity for the mutant allele, and the presence of phenocopies (diseases associated with disruption of other proteins included in the dystrophin glycoprotein complex ). In about 2/3 of cases, the son receives a chromosome with damage from the mother-carrier, in other cases the disease occurs as a result of a de novo mutation in the germ cells of the mother or father, or in the precursors of these cells. Duchenne muscular dystrophy (DMD) occurs in about one in 2,500 to 4,000 newborn boys.
The DMD gene, which is responsible for progressive Duchenne / Becker muscular dystrophy (DMD / BMD), is located at the Xp21.2 locus and has a size of 2.6 million bp. and consists of 79 exons. In 60% of cases, mutations leading to DMD / BMD are extended deletions (from one to several tens of exons), in 30% of cases - point mutations, and in 10% of cases - duplications. Due to the presence of so-called "hot spots" of deletions, the amplification of 27 exons and the promoter region of the DMD gene makes it possible to detect approximately 98% of all large deletions. The search for point mutations is difficult due to the large size of the gene and the absence of major mutations.
At the Center for Molecular Genetics, the level of CPK in the blood is measured, as well as direct diagnosis of DMD / BMD, which is a search for large deletions / l-duplications in all exons of the DMD gene and the search for "point" mutations of the DMD gene using the NGS method (next generation sequensing). Research by the NGS method also makes it possible to detect deletions of all exons of the DMD gene in sick boys. Analysis of all exons of a gene allows one to determine the exact exon boundaries of a deletion in the event of its detection, and thus, to establish whether this deletion leads to a shift in the protein reading frame, which in turn is important for predicting the form of the disease - Duchenne or Becker muscular dystrophy. Thus, the combination of various research methods allows detecting almost all mutations in the DMD gene.
The presence of any type of mutation (deletion / duplication in one or several exons, "point" mutations) is a molecular genetic confirmation of the clinical diagnosis of Duchenne / Becker muscular dystrophy and allows prenatal diagnosis in this family.
Attention! To measure the CPK level, blood must be fresh (not frozen)!
In the case of prenatal diagnosis, fetal biomaterial is required, which can be used as chorionic villi (from 8th to 12th week of pregnancy), amniotic fluid (from 16th to 24th week of pregnancy) or umbilical cord blood (from 22nd weeks of pregnancy).
We have developed. The kits are intended for use in molecular genetic diagnostic laboratories.
When conducting prenatal (prenatal) DNA diagnostics in relation to a specific disease, it makes sense to diagnose frequent aneuploidies (Down, Edwards, Shereshevsky-Turner syndromes, etc.) on the already available fetal material, paragraph 54.1. The relevance of this study is due to the high total frequency of aneuploidies - about 1 per 300 newborns, and the absence of the need for re-sampling of fetal material.