Stages of manufacturing wire tires chlh. Maxillofacial prosthetics
6438 0
A stabilization splint can be made at once (all teeth are immediately covered) and in two stages: first, a palatal plate with a platform behind the front teeth is made (muscle relaxation device), then occlusal overlays are added to the lateral teeth (stabilization device).
Simultaneous production of the splint provides for its modeling with wax on the model with the creation of all the necessary elements: the base, occlusal overlays, elevation in the canine area for "canine guidance".
The splint is made in the central ratio of the jaws, therefore, in the clinic, the central ratio of the jaws is fixed with blocks of hard wax. On the model of the upper jaw, the boundaries of the splint are marked and parallelometry is performed.
Undercuts should be isolated with wax or quick-hardening plaster, as well as palatal gingival papillae. You can make wire retention clasps from the vestibular side. Then the model is installed in the articulator, the splint base and occlusal linings are modeled with wax. To create "canine guidance", the location of the canine is marked on the wax. Then, elevation is modeled with hard wax for inlays. Check the movement of the lower jaw forward and to the side. In the simulated area of the canine, the lateral teeth should be separated in lateral occlusions.
The bite pad for the canines and incisors of the lower jaw should be perpendicular to the axis of the teeth.
For good retention, the edge of the tire on the vestibular side overlaps the line of sight of the lateral teeth by 1-2 mm, and on the palatal side, the alveolar processes up to the last molar.
After modeling is completed, the wax is replaced with plastic. The finished tire is fitted on the model.
A day after the imposition of the finished splint, its correction is necessary. Dropping the splint during lateral movements is a sign of a too steep guiding plane of the palatal surface of the canine, therefore, when correcting, it is necessary to reduce the slope of this surface.
Two-stage tire manufacturing. On the model of the upper jaw, a plate is modeled with overlapping of the palate, the palatine surface of the lateral teeth and the cutting edges of the incisors and canines, with a bite platform from canine to canine. The inclination of this platform is adjusted in the articulator when simulating forward movements of the lower jaw: uniform contact of the platform with the lower incisors, separation of the lateral teeth. In this way, the articular heads can be set in the correct position regardless of occlusal disorders.
The bite pad is modeled so that there is separation of the lateral teeth by 1-2 mm. With all movements of the lower jaw, there should be uniform multiple contact between the bite pad and the lower incisors.
In the central relationship, there should also be no contact of the lateral teeth. After 3-4 days, the effect of relaxation of the masticatory muscles usually occurs and the central ratio of the jaws can be re-determined with a bite block. This makes it possible to establish a new position of the lower jaw in the articulator. Only after that, occlusal overlays are formed on the lateral teeth. While the self-hardening plastic has not hardened, the lower jaw is placed in a central relationship. The occlusion of the posterior teeth is limited by the contact of the bite block with the lower teeth. After complete hardening of the plastic, the occlusal surface is corrected using articulating paper. The final correction (minimum) is carried out in the oral cavity. In lateral occlusions, there should be no contact of the posterior teeth.
Tire manufacturing steps:
In the clinic, impressions are made from both jaws (you need to “shine” the sky!), a facial arch is installed, a block is formed that fixes the central ratio of the jaws; at the next stage, the models are installed in the articulator;
In the laboratory, models are cast, teeth and palate are treated with an insulating substance (for example, silicone vaseline).
For molars and premolars, one-arm clasps are made (wire diameter 0.8 mm), which are strengthened in the sky with transparent plastic.
A plate 2-3 mm thick is prepared from transparent plastic and applied after the beginning of the hardening of the plastic on the model of the upper jaw. When the plastic is in a rubbery state, the lateral teeth are released to the equator, without touching the plastic from canine to canine. The labial surface of the upper incisors and canines is covered with plastic by 2 mm.
Excess plastic must be cut off with a scalpel. Close the dentition in a central ratio to get the impressions of the front lower teeth, and in the lateral areas there should be a gap of 1-2 mm. Wait for the end of the polymerization of the plastic. Place the model of the upper jaw in hot water until the plastic polymerizes completely. Remove the plate without damaging
model teeth. Mark the depressions of the lower teeth on the bite pad. Verify movements in the articulator. Do not polish the plate. Mark on the inner surface of the plate a strip 3 mm wide in the region of the gingival margin and grind off the excess plastic;
In the clinic:
Fitting the plate, checking the centric and eccentric contacts in front of them of the lower teeth from the bite pad and minimal separation of the lateral teeth. If there is no such separation, add plastic in the area of the bite pad;
In the clinic: after removing the pain syndrome, a new bite block is made, fixing the central ratio. If the doctor removes the plate, then he lays cotton rolls between the lateral teeth;
In the laboratory:
Mounting the lower model in the articulator using a new block. After the plastic has hardened, the lateral movements must be checked. In the central ratio should be
multiple contact of the lateral teeth of the lower jaw with occlusal pads; in the clinic: fitting the plate, checking occlusal contacts in the central ratio and with all movements of the lower jaw.
If pain occurs on one side while using the splint, the contacts on that side should be strengthened, not removed, as the cause of the pain is better contacts and chewing on the opposite side.
In case of degenerative processes in the joint, it is additionally necessary to use other methods of treatment (physiotherapy, medicines).
The use of tires can be combined with physiotherapy, myogymnastics, thermal procedures,
Unloading therapy (autogenic training, muscle relaxation exercises, self-observation, psychotherapy).
Manufacture of a vacuum splint for the lower jaw (device "Bio-star"). The size of the plate (thickness 0.6 mm) should be such that, after vacuum pulling, the splint overlaps the gum line by 1 cm.
After vacuum pulling, the tire must remain under pressure for 1 minute.
The tire is removed from the model, cut in a straight line just below the level of the gum. Outside, the blank tire is treated for 5 s in a sandblasting machine with aluminum oxide particles from a distance of 10-15 cm until a matte surface is obtained. In the area of the included defects, insulation is made with silicone, and in the area of the end defects of the dentition, gypsum rollers are formed, after squeezing the splint, the gypsum is removed and the fit of the splint to the alveolar process is clarified with the help of plastic. In order not to damage the anterior teeth of the plaster model, food foil is applied to them before vacuum pulling.
After compression, the model is installed in the articulator and the closure with the teeth of the upper jaw model is checked. If there is supercontact on the third molars, trim the distal margin, leaving a portion of the occlusal surface of the third molars.
Then, a roller is made from the self-hardening plastic "Palapress vario", which is laid on a blank bus. Previously, the teeth of the upper jaw are isolated with silicone A (fissures are closed) and lubricated with an insulating agent "Aislar" ("Kulzer"). The cutting pin is extended by 2 mm. The articulator is closed, the model with the tire is removed and the plastic is polymerized for 20 minutes at a pressure of 1 bar and a water temperature of 55-65 °C. Then the tire is processed, the contacts of the teeth are verified by means of articulating paper. The contact area of the support tubercles is minimal. The protrusion of the tire from the vestibular side of the incisors is made concave (pear-shaped cutters). In anterior occlusion, there should be contact of the upper teeth with the anterior edge of the concave area, in lateral occlusions, the canines should be in contact with this area.
Before using bite plates and occlusal splints, the patient should be informed that:
The tire can cause increased salivation, a change in taste sensations;
with a splint at rest, there should be a gap between the teeth;
outside the mouth, store the tire in a damp cloth and a closed vessel;
bite plates and splints require constant medical supervision and correction;
with increased pain, the splint can be removed;
tires require constant hygienic treatment, as well as removable dentures;
It is not possible to pre-determine how long the tire will be worn. "Be patient, visit your doctor for re-corrections, even if it seems to you that there is no change."
V.A. Khvatova
Clinical gnathology
Topic: Manufacture of splints and prosthetic splints. Demonstration of tire manufacturing (Vankevich, Tigerstedt).
Purpose of the lesson: to teach students the features of orthopedic treatment of traumatic injuries of the maxillofacial region. To characterize and determine the indications for the use of splinting, repositioning and shaping devices. To study the clinical and laboratory stages of their manufacture.
^ Questions needed to master the topic:
The muscular system of the maxillofacial region.
Features of blood supply and innervation of the maxillofacial region.
Test questions:
Devices used in maxillofacial orthopedics, their classification, indications for use.
Classification of fixing devices.
Stages of manufacturing Weber tires, Port tires.
Sheena Vankevich. Indications. Manufacturing stages.
Tigerstedt tires. Indications. Manufacturing stages.
Characteristics and clinical and laboratory stages of manufacturing splints and prostheses used for fractures of the upper jaw (Guning, Oksman).
Classification of devices used in maxillofacial orthopedics:
By function:
Fixing (provide functional stability of fragments).
Repairing (provide gradual reposition of fragments).
Formative (provide temporary support for the shape of the face, create a rigid support, prevent cicatricial changes in soft tissues, deformation of the prosthetic bed, etc.).
Substituting (perform the function of replacing congenital and acquired defects).
Combined (a single design for reposition, fixation, formation and replacement).
Intraoral (single jaw, double jaw, intermaxillary).
Extraoral.
Intra-extraoral.
Standard.
Individual.
Intraoral:
Tooth splints (wire aluminum splint, soldered wire splint on rings (crowns), plastic splints that fix dental devices during osteoplastic operations);
Dental splint (Weber splint);
Suspended gums (monoblock, Port bus).
Extraoral (chin sling with head cap).
Combined (bent aluminum wire splint with a head cap for the treatment of fractures of the upper jaw).
^ Scheme of OOD on the topic: "Clinical and laboratory stages of manufacturing splints and splints-prostheses"
| Name of tire, prosthesis | Materials, tools necessary for manufacturing. Manufacturing steps | Indications |
| Tigerstedt tire smooth | Aluminum wire 2 mm, bronze-aluminum wire 0.3 mm, crampon tongs, file | With easily straightened fractures of the alveolar process of the upper jaw and the presence of at least 2–3 stable teeth on the fragments |
| Tigerstedt busbar with spacer bend | Same A spacer bend is made in the area of missing teeth | For fractures in the edentulous area of the jaw |
| Tigerstedt bar with toe loops | Same | If necessary, the imposition of rubber traction |
| Sheena Vankevich | Acrylic resin base, artificial teeth if necessary, mandibular pads | For various fractures of the lower jaw for fixation and reposition |
| Tire made of stamped crowns connected by two tubes and two pins | Consists of 2 stamped mouthguards (steel grade 1X18H9T) for chewing groups of teeth, on one mouthguard from the lingual and vestibular sides 2 soldered tubes, on the other 2 rods | Unilateral jaw fracture |
| Open vestibular-palatal plate with bushings for extraoral rods | The apparatus is strengthened with extraoral rods on an orthopedic plaster cap | In case of fractures of the upper jaw with a defect and a small number of supporting teeth |
| Cap splint with a sleeve on which the supporting buccal plate is strengthened with a rod | The plate is created by free modeling, an intact jaw serves as a guide for its size and shape. In the middle of the surface adjacent to the cheek, a 1 mm high roller is modeled, which forms a channel in the scar tissue and serves as a support for the prosthesis | With a unilateral fracture of the upper jaw with a defect and a sufficient number of supporting teeth |
| Ring tooth splint according to Limberg | Sleeves (rings), soldered to crowns or rings, an arc of orthodontic wire 1.5–2 mm thick. Fixation of rings on stable teeth, taking impressions with rings, casting models, soldering the splint, whitening, polishing, fixing on teeth. | In case of fractures of the upper jaw with insufficient number of teeth, low clinical crowns |
| Open supragingival splint with repositioning loop, fixed with extraoral rods on a plaster orthopedic cap | A model is cast on the cast, on which the size of individual fragments is clearly outlined. Cannulas for extraoral rods are placed on the vestibular surface of the splint. On the extraoral rods, 2–3 loops are bent on each side for attaching the aluminum wire to the head plaster cap | Bilateral fracture of the upper jaw with a large number of teeth on the jaw and no palate defect |
| Zbarzh standard set | Steel intraoral wire splint, extraoral rods, supporting headband, side metal strips, 4 connecting rods, 8 connecting clips, ligature wire, clips, crown scissors. Preparation of the splint with forceps and pliers in accordance with the individual anatomical features of the dentition. Fixation of the intraoral wire splint to the teeth with a ligature wire. Applying a headband. With an edentulous jaw, a splint-arc is used as a base on which a plate of self-hardening plastic can be applied. | Subbasal fractures of the upper jaw with displacement in the presence of a large number of teeth (superimposed for 2–3–5 weeks). Combined fractures of the upper and lower jaw (wire splint with hook loops on the lower jaw). |
| Sheena Gunning Tire Limberg | Collapsible, strengthened on the teeth with clasps. On the occlusal surface of the lower jaw, splints are made with spikes, on the occlusal surface of the upper part of the recess for them. After the next introduction of splints and fixation of the lower jaw with a chin sling, a lock is formed. | Fractures of the lower jaw in the presence of one or more teeth that do not allow the insertion of the Port splint |
| Bus Port | Impression material, base wax, gypsum, spirit lamp, wax spatula, 2 cuvettes, impression spoons. Taking impressions, making bases with occlusal rollers, determining the central ratio of the jaws, a plaster model in the occluder, modeling the splint with a wax monoblock with a hole in the frontal area 1.5 x 2.5 cm for eating. Replacing wax with plastic. Used in combination with a sling dressing | For fractures of the edentulous upper and lower jaws without displacement |
| Apparatus for repositioning the upper jaw | Steel rod 2.5–3 mm thick, soldered to a plate 30 cm long. Aluminum wire 2 mm thick, rubber band, gypsum, bandage. Reposition of fragments of the upper jaw forward is achieved by an extraoral rod, fixed on a plaster cap. A pre-prepared intraoral splint is pulled up to it. When fragments are piled up, a tooth splint with a loop is installed. Reposition upwards is achieved by applying a rubber band between the plaster cap and the extraoral rods. With unilateral displacement of the jaw, a good reposition can be obtained by installing a rubber gasket between the teeth of the fragment and the antagonists. Traction is carried out between a soft head cap and a sling. | Displaced fractures of the upper jaw |
^ Tire manufacturing Vankevich M.M.
Tire Vankevich consists of the upper base, which is strengthened on the upper jaw. With an edentulous upper jaw, the splint is the basis of the prosthesis, which is fixed on the jaw due to adhesion and the valve zone. If there are teeth, the basis is made in the form of a Weber splint. Vertical processes are welded to this basis, which descend downward, touch the outer surfaces of the lingual surfaces of the fragments of the lower jaw and, thus, hold the fragments in the correct position.
If the treatment was carried out correctly and the movable fragments with single teeth can be separated and set in the correct position, the splint is made immediately together with the supporting planes.
In case of edentulous fragments, the maxillary plastic template is first made from an impression and checked. To set each fragment in the correct position, a buffer from a softened impression mass is attached to the opposite surface of the template. When the patient presses the retracted fragment against the maxilla, the outer surface of the buffer is contoured according to the surface of the retracted fragment. Upon completion of molding and finishing, the impression mass is replaced with AKP-7 plastic.
When the fragments are fused in the wrong position, a maxillary splint is made with a reference plane for one of them at its maximum abduction, without taking into account the displacement of the other fragment. After a trial wearing of the splint, it is installed on a plaster (casting), then, after the plaster has hardened, the tested reference plane with a minimum part of the maxillary splint is sawn off and drawn up on the model. On the most part of the splint removed from the model, a support for the fragment is formed on the other side, also with its maximum retraction and without taking into account the position of the other fragment. After welding, this second formed part of the tire is checked by trial wear. Then both separately tested parts are installed on a gypsum grout and welded together. In this form, with a wide standing of the supporting planes, the splint can be applied only after complete dilution of the fragments with the help of surgical intervention.
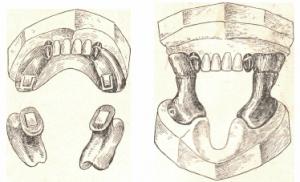
Intraoral apparatus Vankevich for reduction and fixation of fragments of the lower jaw: A - apparatus on the model; B - no model.

Apparatus for intraoral fixation of fragments of the edentulous lower jaw in the absence of chewing teeth in the upper jaw (according to the author): A - details of the apparatus; B - apparatus on the model.
^ Manufacture of Tigerstedt tire.
For more than 80 years, bent wire tooth splints have been successfully used, developed back in the period of the First World War by the dentist of the Kiev military hospital S.S. Tigerstedt (1915). They proposed a large number of different tire designs: a simple brace (now called a smooth brace tire), a support brace (a tire with hook loops), a retention brace (a tire with a spacer bend), various options for brackets with planes, tires with inclined planes and hinges , with levers of various principles of action for moving fragments in chronic fractures, fixation seals, anchor brackets, etc. As the author himself pointed out, his system allowed “...quickly, without casts, without models, without rings, nuts and screws, without soldering and stamping, without vulcanizing do whatever it takes."
Tigerstedt tires have made a real revolution in domestic and foreign traumatology. This was due to the fact that this method of therapeutic immobilization is characterized by relatively low trauma, simplicity, high efficiency and low cost of the materials used.
Over time, in the process of clinical selection, the following bent wire tooth splints have been preserved and successfully used: a smooth brace splint, a splint splint, a splint with toe loops, and very rarely an inclined plane splint.
The following materials are required for the manufacture of tooth splints: aluminum wire with a diameter of 1.8–2 mm and a length of 12–15 cm (in case of high rigidity, it must be calcined and cooled slowly); bronze-aluminum wire with a diameter of 0.5–0.6 mm or stainless steel wire with a diameter of 0.4–0.5 mm; tools: crampon forceps, anatomical tweezers, Billroth hemostatic forceps (without teeth) or Kocher (with teeth), dental scissors for cutting metal, file.
General rules when applying tooth splints:
Subcutaneously administer 0.5 ml of a 0.1% solution of atropine for ease of work due to a decrease in salivation;
Perform local anesthesia, preferably conductive;
Start bending the tire on the left side of the patient's jaw (for left-handers - on the right); some authors recommend starting the bending of the tire from the side of the fracture;
Bend the tire with the fingers of the left hand, holding the wire in the right hand with kampon tongs (for left-handers - vice versa);
Crampon tongs should be placed on the border of the wire (blank) and the curved section of the tire, protecting it from deformation;
After fitting the splint to the teeth, bend it only outside the oral cavity;
The made splint must necessarily adjoin each tooth at least at one point and be located between the gingival margin and the equator of the tooth;
Fix the tire to each tooth included in it with a ligature wire;
Twist the ligature wire only in the direction of clockwise movement (as all doctors agreed).
This ensures continuity when caring for the tire, tightening and loosening the ligature.
Start making a tire by bending a large toe hook or toe spike. When bending the tire, the aluminum wire is fixed with crampon tongs, and it is bent by pressing the wire with your fingers to the cheeks of the tongs to avoid deformation of the part of the tire fitted to the teeth. The splint is tried on in the mouth and bent outside the patient's mouth. To try on a curved section of the tire, it is applied to the patient's teeth and fixed with the fingers of the right hand in the area of the large hook or hook spike, i.e. in the area of the already manufactured tire. This condition is very important. Do not try on the splint by holding it by the section of wire protruding from the mouth, as this leads to incorrect placement of the splint on the teeth. Having made a splint on one half of the jaw, they proceed to bending it on the other half. In this case, the long end of the wire of the workpiece must be bent by 180 °, leaving its piece sufficient to make the second half of the tire.

Wire bus according to Tigerstedt: a - wire arch and ligature; b - the position of the arc with defects; c - hook loops; g - shift limiter; e - rubber rings and intermaxillary traction.
^ Situational tasks
The patient is 72 years old. Fracture of the edentulous upper jaw. The radiograph revealed a subbasal fracture. Determine the type of orthopedic treatment.
A 25-year-old patient was delivered to a dental clinic with a suborbital fracture of the upper jaw on the right. Explain the options for orthopedic treatment.
The patient is 50 years old. He was admitted to the clinic with a fracture of the upper jaw Le Fort 1. There are partial defects in the dentition on the jaw. Small clinical crowns. Justify the plan of orthopedic treatment.
A 55-year-old patient, a simultaneous fracture of the upper and lower edentulous jaws. Make a plan for orthopedic treatment.
A 20-year-old patient was admitted with an unexplained fracture of the upper jaw. There are partial defects of the dentition on the jaw. Justify the plan of orthopedic treatment.
The patient is 38 years old. Was admitted with a diagnosis of fracture of the body of the lower jaw with displacement. There are partial defects of the dentition on the jaw. Make and justify a plan of orthopedic treatment.
Literature
Lecture material of the Department of Orthopedic Dentistry of Belarusian State Medical University.
Gavrilov E.I.,0ksman I.M. Orthopedic dentistry. 1978, pp. 401–408, 411–417.
Gavrilov E.I., Shcherbakov A.S. Orthopedic dentistry. 1984.
Kabanov B.D., Malyshev V.A. Jaw fractures. M., 1981.
Kopeikin V.N. Orthopedic dentistry. 1988, pp. 463–470.
Kurlyandsky V.Yu. Atlas II vol., pp. 269–275, 282–285, 297–320.
Kurlyandsky V.Yu. Orthopedic dentistry. 1977, pp. 410–417.
Tigerstedt tires. Tooth wire splints were developed by S.S. Tigerstedt in 1915. Several designs were proposed.
This method of therapeutic immobilization is characterized by low trauma, simplicity, high efficiency and low cost of the materials used.
The following Tigerstedt splints are currently in use: a smooth shackle splint, a spacer bent splint, a hook-and-loop splint, and very rarely an inclined plane splint.
For the imposition of dental individual wire splints, you need:
Materials - aluminum wire with a diameter of 1.8-2.0 mm and a length of 12-15 cm (in case of high rigidity, it must be calcined); bronze-aluminum wire with a diameter of 0.5-0.6 mm or stainless steel wire with a cross section of 0.4-0.5 mm;
Tools - crampon tongs; anatomical tweezers; Billroth, Pean or Kocher hemostatic forceps; dental scissors for cutting metal; file.
General rules to be observed when applying dental splints:
Subcutaneously inject 0.5 ml of a 0.1% solution of atropine to reduce salivation (convenient for the doctor and the patient during the manufacture of the tire);
Conduct local anesthesia, preferably conductive;
Remove tartar for free passage of the wire ligature in the interdental spaces;
Start bending the tire from the left side of the patient's jaw (for left-handers - from the right), some authors recommend starting bending the tire from the side of the fracture;
The tire is bent with the fingers of the left hand, holding the wire in the right hand with kampon tongs (for left-handers - vice versa);
Try on the splint to the teeth in the mouth, and bend it only outside the oral cavity;
The manufactured splint must be adjacent to the neck of each tooth included in it, at least at one point;
The tire should be fixed to each tooth included in it with a ligature wire;
It is necessary to twist the ligature wire only clockwise (as all doctors agreed). This ensures continuity in the care of the tire and its safety when tightening and loosening the ligatures.
Manufacturing technique. Splint making begins by bending a large toe hook that wraps around the first tooth, or a toe spike inserted into the interdental space. The aluminum wire is always fixed with kampon tongs, and bent by pressing the fingers of the hand against the cheeks of the tongs in order to prevent deformation of the section of the tire fitted to the teeth. To try on the curved section of the tire, it is applied to the teeth and fixed with the fingers of the left hand in the area of the toe hook or spike, i.e. in the area of the manufactured tire. It is not recommended to try on the splint by holding it by the section of wire protruding from the mouth, as this may lead to incorrect placement of the splint on the teeth. Having made a splint for one half of the jaw, they proceed to bending it to the teeth of the other half. In this case, the long end of the wire will interfere with the manufacture of the splint on the opposite side, so it must be bent 180° to enable the wire to fit (bend) to the teeth of the opposite side.
A. Smooth busbar
It is used to treat fractures of the lower jaw, provided that there are at least 4 stable teeth on the larger fragment, and at least 2 on the smaller one (Fig. 8-7). Teeth located in the fracture gap are not taken into account in this rule.
Indications for use:
Linear fractures of the lower jaw, located within the dentition, without displacement or with easily reducible fragments;
Fractures of the alveolar part of the lower jaw and the alveolar process of the upper jaw;
Rice. 8-7. Smooth busbar
Fractures and dislocations of teeth, when there are stable teeth on both sides of the intact areas of the jaw;
Acute odontogenic osteomyelitis of the jaw and periodontitis;
Fractures of the upper jaw (using the methods of Adams, Dingman, etc.);
As a method of preventing a pathological fracture of the lower jaw prior to certain operations (sequestrectomy, cystectomy, cystotomy, resection of a part of the jaw, etc.).
Method for bending a smooth bus-bracket. If there is a displacement of the fragments, then before bending the splint, it is necessary to compare them with your hands and temporarily fix them with a wire ligature for the teeth of the fragments facing the fracture gap.
For splinting, a piece of aluminum wire is taken in the left hand and with crampon forceps in the right hand, the toe hook is bent to the wisdom tooth (or to any last tooth in the dentition). When making a hook, the wire is bent at a slight angle, each time capturing new sections of the wire with tongs, successively retreating from the end by 1-2 mm. The hook should tightly cover the distal and buccal surface of the last tooth, reach the middle of the crown of its lingual surface and be located between the equator and the edge of the gum.
The lingual end of the hook is sharpened with a file at an angle of 45 ° for a smooth transition of the wire to the tooth surface, which eliminates injury to the tongue.
Sometimes, instead of a toe hook, the bending of the tire begins with the manufacture of a toe spike, which should enter the interdental space, but not protrude into the oral cavity and not injure the interdental papilla.
After manufacturing, the hook is placed on the last tooth and the wire is grasped with forceps at the level of the middle of its crown from the vestibular side. In this case, the long end of the hook (the main part of the wire) will be significantly lowered down and not correspond to the projection of the dental arch (Spee curve). The tongs, when applied to the wire, should be horizontal. With kampon tongs, remove the hook from the tooth and with the second finger of the left hand at the cheeks of the tongs, bend the wire up at a small angle.
Try on the tire in the mouth, applying it to the teeth.
If the bending angle was correct, then the wire after the last manipulation will be at the level of the necks of several teeth.
If the wire is above or below their necks, it must be bent down or up to the appropriate angle so that it is in the projection of the necks of several teeth. Then it is captured with forceps at the last point of contact with the tooth, removed and carefully removed from the mouth. Slightly loosening the fixation of the forceps, turn them on the wire with the handles down by 90 ° and bend the wire away from you with the first finger of your left hand to the next tooth at a small angle. A splint is inserted into the vestibule of the mouth and tried on to the teeth. If it turns out that after bending the wire to the tooth, the correctly curved section of the splint moved away from the teeth, then this means that the wire was bent excessively. To correct it, you need to put forceps on the wire at the last bend and bend it slightly away from the tooth, i.e. on itself, and again try on the tire to the teeth in the mouth, hooking it on the last tooth. If the position of the splint is correct, then with the cheeks of crampon forceps again grab the splint at the place of the last touch to the tooth, remove it from the vestibule of the mouth and continue to bend in the direction of the occlusal plane until it contacts the next tooth.
In a similar way, repeating the manipulations, the entire tire is sequentially bent to the required length and its bending is completed at the second fragment with a hook or spike, which is inserted into the interdental space. To bend the spike, the wire is grasped with forceps exactly at the level of the back surface of the selected tooth, the splint is removed from the teeth and removed from the mouth. Slightly loosening the fixation of the forceps, turn them on the wire with their handles down by 90 ° and bend the wire away from you with the first finger of your left hand by 90 °. Cut off the excess wire, leaving the end for a spike measuring 3-6 mm. With the help of a file, the spike is processed, giving it the shape of a wedge so that it enters the interdental space. The size of the spike corresponds to the size of the interdental space, and the spike itself should be located just above the interdental papilla, not injure it and not protrude with a sharp end into the oral cavity. It should be noted that sometimes the teeth are so tight that the size of the spike does not exceed 1-1.5 mm.
Try on the finished tire in your mouth. For the convenience of applying the splint, first a spike is inserted into the interdental space, and then the entire splint is put on the teeth, hooking the hook on the first tooth. A properly made splint should easily and effortlessly overlap the vestibular surface of the dental arch. It should touch all the teeth at least at one point and be located between the equator of the tooth and the edge of the gum.
The finished tire is tied to each tooth with a bronze-aluminum wire. To do this, before applying the aluminum tire, the wire is grasped with tweezers or a clamp, departing from its end by 2-3 cm, and it is inserted from the vestibule into the oral cavity through the interdental space. Next, the oral end of the wire is grasped with a clamp and it is brought out through another interdental space in the vestibule of the mouth, surrounding the tooth from the distal, lingual and medial sides. The wire should be below the equator of the tooth. The distal end of the wire is bent up, and the medial end is down. Between these ends (they should be approximately equal in size) a space is formed where the curved tire will subsequently be placed. When passing the wire into the oral cavity, it is necessary to protect the tongue from injury with the wire. To do this, with the second finger of the left hand, the wire is bent to the teeth as it moves into the oral cavity.
In a similar way, wire ligatures are applied to all teeth included in the splint. All distal ends are folded up, and the medial ends are bent down. After the ligatures are applied, the tire is fixed. It is applied to the teeth, introducing between the ends of the wire ligatures. The upper and lower ends of the wire ligature of each tooth are twisted clockwise, capturing them with a clamp at a distance of 2.0-2.5 cm from the vestibular surface of the crown.
In order not to confuse the upper end of one ligature with the lower end of the other, they must be shaken before twisting. With this movement of one end in the oral-vestibular direction, the paired end of the same ligature moves synchronously.
After twisting the ligatures, each of them is cut to a length not exceeding 5 mm, and the ends are bent to the tire or to the teeth towards the midline. It is necessary to ensure that the ends of the ligatures do not injure the surrounding tissues.
You can fix the tire to the teeth in another way. To do this, the splint is fixed on the teeth with a spike and a hook. The wire ligature is bent in the form of a hairpin and its ends are inserted from the oral cavity: one into the medial, the other into the distal interdental spaces of the same tooth. In this case, one end of the wire (for example, medial) is carried out under the tire, and the other (distal) - above the tire. The wire is not twisted to the end, leaving the tire movable to facilitate subsequent ligatures. Similarly, ligatures are applied to all teeth. All ligatures are tightly twisted, cut and folded
ends to the teeth, as above. This method often causes difficulties when conducting, as a rule, the upper end of the ligature, which abuts against the inner surface of the tire.
After treatment, before removing the splint, loosen the ligatures and check the lack of mobility of the fragments by shaking them.
The splint is removed after 4-5 weeks. To do this, the ends of the wire ligatures are slightly untwisted with crampon tongs counterclockwise, one or both of them are cut with scissors for metal and the wire is removed from the interdental space. If the ligature jams, it must be slightly shifted towards the gums, pushed into the oral cavity and then removed. The tire is removed from the teeth, the gum is treated with a 3% hydrogen peroxide solution or 1% iodine solution.
After applying a smooth splint-bracket, the patient is recommended to wear a standard Pomerantseva-Urban chin sling to limit mouth opening. The patient needs to take liquid or pureed food. The doctor should regularly examine the patient 2-3 times a week. At the same time, it is necessary to control the state of bite, the strength of fixation of bone fragments with a splint, the state of tissues in the area of the fracture (the presence or absence of inflammation), the state of the teeth in the fracture gap.
When loosening the fixation of the splint on the teeth, it is necessary to tighten the ligatures by twisting them clockwise. If at the same time the ligature bursts, it is replaced with a new one.
Of particular importance is the condition of the oral cavity. The patient must be taught hygiene measures to prevent the development of gingivitis. To this end, the patient should brush his teeth and the splint with toothpaste and brush 2 times a day (morning and evening), after each meal, remove food debris with a toothpick and rinse the cavity and vestibule of the mouth with antiseptic solutions 3-5 times a day: pink potassium solution permanganate, decoctions of sage or chamomile, etc.
B. Clamp bar with spacer bend
This splint can be used if there are at least 2 stable teeth on the smaller fragment, and 4 on the larger one. The spacer bend prevents lateral displacement of the fragments (Fig. 8-8).
Indications for use:
Fracture of the lower jaw within the dentition and the presence of a bone defect of no more than 2-4 cm;
 Rice. 8-8. Cleat rail with spacer bend
Rice. 8-8. Cleat rail with spacer bend
Fracture of the lower jaw without displacement or with easily reducible fragments, if the fracture gap passes through the alveolar part, devoid of teeth.
The same materials and tools are needed for bending a brace with a spacer bend as for making a smooth brace.
The method of bending a tire with a spacer bend differs from the manufacture of a smooth brace only at the stage of forming the spacer. Strut length
should correspond to the length of the defect in the bone or dentition. Otherwise, there will be an increase or decrease in the length of the lower jaw. The shoulders of the spacer bend, abutting against the teeth, must be equal to the supporting surface. This must be taken into account when bending the spacer and make allowance for the thickness of the wire, since it takes part in the formation of the shoulder.
To bend the spacer bend, the cheeks of the forceps are placed on the busbar parallel to the surface of the tooth facing the defect, and, having removed the splint from the teeth, the wire is bent away from itself at an angle of 90°. The long end of the wire is smoothly bent towards itself in the form of a semicircle until it is oriented towards the exit from the oral cavity, the splint is tried on and the wire is grasped with forceps at the level of the lingual surface of the tooth. You can do it differently: make a mark-scratch at this level. Then the splint is removed, the cheeks of the forceps are displaced from the place of capture (or mark-scratches) in the vestibular direction by the thickness of the wire and bent 90° towards the defect. The wire is straightened in a section slightly longer than the existing defect. The tire is again tried on and, having removed it from the mouth, the wire is bent over the middle of the defect.
It is necessary to ensure that this segment is not displaced orally, this will exclude injury to the tongue, or vestibularly - this will prevent damage to the mucous membrane of the cheek or lip. This section of the wire must be raised to the upper edge of the crown of the tooth, which is on the other side of the defect, and placed on its oral surface. With a sharp tool, you can make
mark-scratch at the level of the surface of the tooth crown facing the defect, or put the cheeks of the forceps here and remove the splint from the mouth.
Stepping back from the mark or from the place of application of the cheeks of the forceps towards the defect by the thickness of the wire, bend its free end towards itself by 90 °. The splint is tried on, the wire is grasped at the place of the shoulder of the spacer bend brought out at the border of the medial and vestibular surfaces of the tooth crown and removed from the mouth. Turning the forceps on the splint by 90° with the handles down, bend the wire away from you until it comes into contact with the vestibular surface of the abutment tooth crown. Further bending and fixation of the splint to the teeth are similar to those described for the brace splint.
B. Bar with toe loops
This tire is most often used to treat patients with fractures of the jaws (Fig. 8-9).
In case of fractures of the lower jaw, 2 splints are made with hook loops for the teeth of the upper and lower jaws.
For fractures of the upper jaw, depending on the method chosen, either one (when fixing the upper jaw to the bones of the upper face) or two splints with hook loops (in the case of using a chin sling) can be used.
 Rice. 8-9. Hook bar
Rice. 8-9. Hook bar
Indications for use:
Fractures of the lower jaw outside the dentition;
Fractures of the lower jaw within the dentition in the absence of 4 stable teeth on the larger fragment, and two on the smaller one (otherwise, the periodontium used for splinting teeth may not withstand the load, and the teeth will become mobile);
Fractures of the lower jaw with fragments that are difficult to reduce and require traction;
Bilateral, double and multiple fractures of the lower jaw, fracture of the upper jaw (with the obligatory use of a chin sling);
Simultaneous fractures of the upper and lower jaws (complemented with a chin sling).
Tire bending technique with toe loops. They take a piece of aluminum wire 15 cm long in the left hand and with the help of crampon forceps in the right hand, bend the hook on the wisdom tooth (or on the other last tooth in the dentition). The hook is bent and sharpened as in the manufacture of a smooth brace.
They bend the tire to the next tooth (let's say it will be the second molar). The tire should touch the second and third molars at least at one point and be located between the equator and the edge of the gum. They grab the splint with forceps in the interdental space of the first and second molars, a little closer to the first molar, remove the splint from the teeth and remove it from the mouth without changing the position of the splint in the forceps.
Next, they begin to bend the toe loop (Fig. 8-10). Holding the forceps with the handles upwards, the cheeks are placed on the splint at an angle of 30-40° with respect to the vertical axis of the tooth. The splint is removed from the mouth, the tongs with the pinched splint are placed in a vertical position with the handles down, and the first finger of the left hand is bent the wire away from itself by 90°, pressing firmly against the cheeks of the tongs.
Holding the bent (long) end of the wire with your left hand, move the cheeks of the tongs onto it, placing it close to the formed corner. With the second finger of the left hand, located near the left cheek of the forceps, turn the long end towards itself (by 180 °), pressing it tightly against the left cheek. The cheeks of the tongs are moved to the base of the loop, its shoulders are brought together and at the same time the long end of the wire is bent away from itself by 90 °, making it a continuation of the already bent part of the tire. The tire is tried on the teeth. The top of the loop on the lower jaw should be turned down, its length is not more than 5 mm, it should be located at an angle of 30-40 ° to the tooth. If the angle of inclination of the loop with respect to
 Rice. 8-10. Scheme of the bending steps (1-4) of the toe loop
Rice. 8-10. Scheme of the bending steps (1-4) of the toe loop
the gingival mucosa is less than 30°, then the toe rubber ring subsequently put on the loop will lead to the formation of a bedsore on the gums. If the angle is more than 45 °, then a bedsore can form on the buccal mucosa.
The criterion for the correct angle of inclination of the loop can be a piece of the wire from which the tire is bent: it must pass between the tooth and the loop, slightly touching them. If the wire does not pass, the loop should be bent; if 2 wires pass, the loop should be bent to the tooth. If the angle between the loop and the tooth does not correspond to the required one, then you can no longer continue to bend the tire. It is required to immediately correct the angle of the hinge. To do this, immediately in front of the loop (in the section of the already bent splint), the wire is grasped with the cheeks of crampon forceps, and the loop is fixed with a hemostatic clamp. Holding the wire tightly with crampon tongs, the hook loop is rotated with a clamp at a small angle, achieving a slope of 30-40 °. Using the experience of bending a smooth brace splint, bend the splint to the second premolar. Toe loops are bent on even teeth, i.e. on the second incisors, first premolars and first molars, if the anatomical conditions and localization of the fracture allow this. Having bent the toe loop to the first premolar, the splint is adjusted to the canine, after which the loop is bent to the second incisor and the splint is bent to the first incisor. After crossing the midline of the lower jaw, continue to bend the tire using the same technology. However, on the opposite side of the jaw, it is necessary to grab the wire to bend the toe loop in front of the tooth on which it should be located. Finish bending the tire by making a hook or spike, using the techniques described for bending the brace.
In a similar way, a splint with hook loops for the teeth of the upper jaw is made, but the hook loops on it should be turned with their top up. At the same time, the wire should be grasped with forceps in such a way that the handles of the forceps are facing downwards, and the angle of inclination is also 30-40° to the buccal surface of the tooth crown. The first movement when bending the loop should be 90 ° towards you.
Toe loops are usually bent on the bar so that they are located in the area of 6, 4 and 2 teeth. If the patient does not have these teeth, then toe loops are made in the area of other teeth, but this must be done in teeth that have antagonists. Usually on a splint adjacent to the teeth of a larger
fragment, bend 3-4 toe loops, and the smaller one - 2-3. The base of the loop must be within the crown of the tooth.
Manufactured splints are placed on the teeth of the jaws and their quality is checked: it is necessary that the splints fit to each tooth at least at one point, the toe loops should form an inclination angle of 30-40 ° to the tooth axis, the toe loops of both tires should be approximately at the same level, the tire should be located between the edge of the gums and the equator.
A splint is attached to each tooth using aluminum-bronze wire as described above.
After fixing the splints on the teeth of the upper and lower jaws, the elastic and smooth movement of the fragments to the correct (normal) position is started. To do this, rubber rings are put on the hook loops. The replicating rubber traction (oblique, vertical or mixed) should be directed in the direction opposite to the displacement of the fragments, taking into account the traction of the muscles and the severity of the fragments. In such cases, the rubber traction separates fragments of the jaw overlapping each other or wedged in their ends in a vicious position in different directions.
You should not create a small thrust for a long time (for several days), as this prolongs the suffering of the patient, gives a smaller effect and leads to tooth mobility. It is better to make anesthesia, apply a powerful rubber traction and reposition the fragments within a short time. The correct reposition of the fragments to which the splint is attached can be judged by the restoration of the correct bite. Then, the traction should be reduced and the fragments should be fixed for the entire period of treatment with the help of rubber rings or wire ligatures. The latter will relieve the periodontium of the teeth included in the splint from non-physiological load.
Sometimes, in case of fractures in the area of the body of the lower jaw, it is more advantageous to tie a curved splint rigidly only to the teeth of the fragment being moved. To the teeth of a correctly standing fragment, the splint is only slightly fixed with ligatures. Reposition in any case will be faster and more successful when the pellet is temporarily placed on the teeth of an undisplaced (or slightly displaced) fragment.
After the fragments are repositioned, the wire ligatures are twisted to a rigid attachment.
When the displacement of the fragments is large and it is not possible to bend one splint onto both fragments, it is possible to make and firmly fix the splints on each of the fragments. After their reposition, rubber rings are put on the toe loops at an angle so that they create a com-
compression of fragments, which significantly prevents their movement. Some authors, after reposition, recommend that such fragments be united with a smooth splint-bracket superimposed over a splint with hook loops. However, this is a complex and not entirely justified procedure. It is best to restore the continuity of the tire with a fast curing plastic placed on the 2 adjacent ends of the tire.
The correctness of the location of the fragments is finally judged by the occlusion and x-ray data, made in at least two projections.
After splinting for a fracture of the upper jaw, it is necessary to put on the patient an elastic chin sling. Otherwise, when opening the mouth, the lower jaw will shift (pull) down the upper one.
Periodically (2-3 times a week), the patient is examined, the fixation strength of the splints is corrected by twisting the ligatures, the rubber rings are changed, as they stretch and fragments can be displaced, and the vestibule of the mouth is treated with antiseptic solutions. They monitor the state of bite, the position of fragments and tissues in the area of the fracture.
10-25 days after the fracture, a dynamic X-ray examination is performed to control the position of the fragments. It is necessary to educate the patient on oral hygiene measures, as described above. Particular attention should be paid to the proper nutrition of the patient.
After the fusion of fragments (determined clinically), before removing the splints, it is necessary to remove the rubber rings and let the patient walk for 1-2 days without fixation (with open jaws), taking soft food. If during this time there is no displacement of fragments, as indicated by a violation of the bite, the tires are removed. If there is a slight change in bite, then the rubber traction is retained for another 10-15 days.
A splint with hook loops can be used as one of the main bearing elements of the surgical method of immobilization of the upper jaw. In this case, the tops of the hook loops of the maxillary splint should be facing down. Usually bend no more than two loops on each side.
G. Splinting according to the method of A.P. Vikhrova and M.A. Slepchenko
 Rice. 8-11. Splinting according to Vikhrov-Slepchenko
Rice. 8-11. Splinting according to Vikhrov-Slepchenko
loops). To do this, take a bronze-aluminum wire ligature, fold it in the form of a hairpin and insert both ends of it into one interdental space from the mouth towards the vestibule of the mouth. The ligature is tightened so that a small loop forms on the lingual surface of the interdental spaces (Fig. 8-11).
Do a similar procedure in the area of all interdental spaces. They take a polyamide thread with a diameter of 1 mm and pass it through all the loops on the lingual side, the ends of the thread are brought out in the vestibule of the mouth behind the last teeth on both sides.
Then, a previously made splint is placed on the teeth so that it is located between the two ends of the same previously made bronze-aluminum ligatures, which are then twisted. According to the authors, the advantages of their method are as follows: a stronger bonding of fragments, a reduction in the time of fixing the splint, and the absence of trauma to the gingival mucosa.
E. Bronze-aluminum wire splints
They are variants of ligature knitting according to the type of machine seam.
Obwegeser method (Fig. 8-12): take a piece of bronze-aluminum or other ligature wire 20-25 cm long. One end of it is placed along the vestibular surface of the dental arch, the other is passed and removed through the same interdental space from the lingual side along towards the vestibule of the mouth, while on the way to the vestibular surface they capture a long ligature wire like a machine seam.
 Rice. 8-12. Intermaxillary ligature fastening according to the Obwegeser method
Rice. 8-12. Intermaxillary ligature fastening according to the Obwegeser method
The protruding wire ligatures are twisted, thereby obtaining hook loops, which are used later to implement rubber traction.
The Stout method differs from the Obwegeser method in that the wire ligatures protruding into the vestibule of the mouth are twisted in the form of a loop using a device.
These methods and others similar to them are time consuming and do not always allow achieving good long-term immobilization, therefore, they are currently used extremely rarely.
Tooth standard splints
Good manual skills are required to make custom wire or plastic splints. In addition, the process of their manufacture requires a lot of time and frequent step-by-step fitting to the dental arch. It is especially difficult to bend splints in case of malocclusion, dystopia of teeth, etc. Given the above, standard splints were proposed, which are manufactured in the factory, do not need to bend the toe loops, and thereby simplify splinting.
In Russia, V.S. Vasiliev. Such a tire is made of a thin flat metal tape 2.3 mm wide and 134 mm long, on which there are 14 hook loops. The tire flexes easily in the horizontal plane, but does not flex in the vertical plane. The Vasiliev tire is cut to the required size, bent along the dental arch so that it touches each tooth at least at one point, and is tied to the teeth with a ligature wire.
The advantages of the splint are in the speed of its application, however, a significant disadvantage is the impossibility of bending it in the vertical plane, which does not allow to avoid injury to the mucous membrane in the lateral parts of the jaws due to the discrepancy between the Spee curve. For single-jaw splinting, this tire is not suitable due to its low strength.
Abroad, there are standard tires of various designs made of steel wire (Winter tires) and polyamide materials that can be bent in any plane. The tires roll easily into a roll and come with pre-made hooks. They are also not strong enough and can only be used for double jaw splinting.
Similar information.
dental wire
splinting,
proposed by S.S. Tigerstedt during the First World War (1916). IN
1967 V.S. Vasiliev developed a standard stainless steel band tire with ready-made toe hooks (Fig. 12
-2).
Rice. 12
-2.
Tires for tooth splinting for jaw fractures: a
- bent wire bus
S.S. Tigerstedt; b
- standard band splint for intermaxillary fixation according to V.S. Vasiliev
Distinguish
bent tires
from wire:
smooth tire
- bracket;
a smooth tire with a spacer;
a tire with hook loops;
a tire with hook loops and an inclined plane;
splint with toe loops and intermaxillary traction. For
splinting the following tools are required:
crampon tongs;
pliers;
anatomical and dental tweezers;
needle holder;
clip;
dental mirror;
file for metal;
crown scissors.
From
materials
needed:
aluminum wire 1.5 thick
-
2 mm in segments of 25 cm;
bronze-aluminum or copper wire, length 5
-
6cm thick 0.40.6cm;
rubber drain tube with 4 holes
-
6 mm for rubber rings;
dressing.
Before splinting, the patient's mouth must be freed from the remnants of food masses, plaque, broken teeth, bone fragments, blood clots with gauze balls soaked in a 3% hydrogen peroxide solution, followed by irrigation with potassium permanganate 1 ÷ 1000. If necessary, conduct anesthesia.
When fitting and applying
aluminum tires
(Fig. 12
-
3) it is necessary to adhere to certain requirements.
The tire should be curved along the vestibular surface of the dentition in such a way that it is adjacent to each tooth at least at one point. It is not necessary to bend it along the contours of the crowns of the teeth.
The tire should not be adjacent to the mucous membrane of the gums in order to avoid the formation of bedsores.
The splint ends are bent in the form of a hook around a distally located tooth in the form of an equator or in the form of a spike and inserted into the interdental space of the distal teeth from the vestibular side.
Rice. 12
-3.
Types of wire busbars: a
-
smooth tire
-
bracket; b
-
tire according to Schelhorn; in
-
wire splint with sliding hinge according to Pomerantseva
-
Urbanskaya; G
-
smooth
wire splint for impacted fracture
The arc is bent with fingers along the dentition with frequent correction in the oral cavity, avoiding repeated bending.
Forcible pressing of the tire to the teeth is unacceptable in order to avoid pain and displacement of fragments.
If there is a defect in the dentition, a U-shaped loop is bent on the splint, the upper crossbar of which corresponds to the width of the defect and faces the oral cavity.
The loops are bent with kampon tongs. The distance between the loops is not more than 15 mm, according to
2-
3 loops on each side. The toe loop should be no more than 3 mm long and bent at an angle of 45° to the gum. Loops should not injure the oral mucosa.
The splint is fixed with ligatures to as many teeth as possible. Ligatures are twisted clockwise, the excess is cut off and folded towards the center so that they do not injure the mucous membrane.
smooth tire
-
brace
shown:
with fractures of the alveolar process, if one-stage reduction of fragments is possible;
with median fractures of the lower jaw without vertical displacement of fragments;
with fractures within the dentition, if it is not accompanied by a vertical displacement of fragments;
with bilateral and multiple fractures of the lower jaw within the dentition, when a sufficient number of teeth are preserved on each fragment.
With the same indications, standard tires V.S. can be used. Vasiliev.
A smooth splint with a spacer is used for fractures with a defect in the dentition.
With vertical displacement of fragments in the event of a fracture within the dentition, tires with hook loops are used.
Tires with intermaxillary traction are used to treat fractures behind the dentition. In the treatment of fractures with vertical displacement of fragments, direct intermaxillary rubber traction is used. For the treatment of fractures with displacement of fragments in two planes, oblique intermaxillary traction is indicated.
In case of fractures of the lower jaw with a small number of teeth on fragments or in their complete absence, extra-osseous extra-oral devices V.F. Rud
- ko, Ya.M. Zbarzha.
In order to simplify the technique of manufacturing dental splints and improve the fixation of fragments of the lower jaw, it is proposed to use a quick-hardening plastic, the main indication for the use of which is the fixation of bone fragments after they have been established in the correct position.
For fractures in the lateral sections, with osteomyelitis of the lateral section, to prevent displacement of fragments in the event of a pathological fracture, a stable inclined plane is used during surgery, which is 2
-
3 crowns made on the lateral teeth of the intact side, or a brazed tire, on the vestibular side of which a stainless steel plate is soldered. The plate rests on the vestibular surface of the teeth
- antagonists of the upper jaw. Its edge should not be higher than the necks of the teeth of the upper jaw with closed teeth, so as not to injure the mucous membrane. The plate is soldered to the crowns of the lower teeth just below the equator so that it does not interfere with the closing of the teeth.
In case of bilateral fractures of the lower jaw with a displacement of the median fragment downwards, the lateral fragments are parted and fixed in the correct position with a steel wire arch, and the short fragment is pulled up with the help of an intermaxillary traction. Treatment ends with a smooth splint
- with a bracket after all fragments are established in the correct closure of the teeth.
In case of a fracture of the lower jaw with one toothless fragment, it is fixed with a bent splint with a loop and a thermoplastic lining. Fragment with teeth is strengthened with wire ligatures to the teeth of the upper jaw.
For the treatment of single fractures of the lower jaw with complete mobility of fragments in the case of a small number of teeth on the fragments or the mobility of all teeth, a removable dentogingival Weber splint is used (Fig. 12
-
4). Such a tire covers the entire remaining dentition and gum on both fragments,
leaving open the chewing and cutting surfaces of the teeth. It can be used for post-treatment of mandibular fractures.
Rice. 12
-4.
Weber bus: a
-
the stage of manufacturing the wire carcass of the tire; b
-
finished tire
In case of fractures of the edentulous lower jaw and the absence of teeth on the upper jaw, devices are used
gunninga
-
Port, Limberg in combination with a chin sling (Fig. 12
-5).
Among fractures of the upper jaw, fractures of the alveolar process are more often noted. They can be without offset and with offset. The direction of displacement of the fragment is determined by the direction of the acting force. Basically, the fragments are displaced backwards or towards the midline.
First aid for treatment
fractures of the alveolar process comes down to setting the fragment in the correct position and applying a sling or outer bandage so that the teeth
- antagonists tightly closed. You can successfully apply an elastic sling bandage.
Simple specialized treatment of fractures of the alveolar process is carried out with a smooth aluminum or steel splint
- bracket. Fragment is repositioned first
Rice. 12
-5.
Devices used to treat fractures of the jaws in the complete absence
teeth: a
-
gunning apparatus
-
Port; b
-
Limberg apparatus
hands and with closed teeth bend the tire with hands
- bracket on the upper dentition. Then, between all the teeth, wire ligatures in the form of hairpins are threaded and their ends are brought out in the vestibule of the mouth. The splint is fixed to the teeth of the intact side, the patient is asked to close his teeth in the correct position, a sling is applied, and then the fragment is tied to the splint
- bracket. The sling is removed after the bracket is fully fixed. If there are contraindications to the tire
- bracket, a full splint is made with the location of the supporting crowns on the teeth of the intact area and the fragment.
At
fractures of the body of the upper jaw
(suborbital and subbasal) with free mobility of fragments, first aid is reduced to establishing the fragments in the correct position and fixing them to the head cap. For this purpose, standard devices are used: tires
- Spoons of Entin, Limberg, hard chin sling. Sling dressings are effective if the lower jaw is not damaged and both jaws have at least 6
-
8 pairs of teeth
- antagonists. Standard tires
- spoons impose on 1
-
2 days Their main disadvantages include: bulkiness, weak fixation of fragments, unhygienic, inability to follow the correct setting of the damaged upper jaw, since the splint
- the spoon covers the entire dentition.
Simple specialized treatment
is reduced to the simultaneous reduction and fixation of fragments in the correct position. For this, individual wire tires are used: solid-bent and composite. Inside
- and extraoral processes
- the levers connected to the tires are fixed in a plaster cap. For the treatment of fractures of the anterior jaw, Ya.M. Zbarzh proposed a solid-bent tire made of aluminum wire (Fig. 12
-6).
For the treatment of fractures of the upper jaw according to the Le Fort type I and II, Ya.M. Zbarzh has developed a standard kit consisting of a tire
- arc, support bandage and connecting rods, which can simultaneously fix and reduce fragments. Complex specialized treatment of a fracture of the upper
Rice. 12
-6.
Apparatus for the treatment of fractures of the upper jaw according to Ya.M. Zbarzhu: a
-
head
plaster cap; b
-
bent wire splint with extraoral processes,
fixed to the head cap
jaws with downward displacement with free mobility of the fragment (suborbital fracture) and the integrity of the lower jaw are carried out using the method inside
- oral fixation with a Weber splint with extraoral levers attached by means of elastic traction to the headband. It covers the teeth and the mucous membrane of the gums around the dentition from the palatine and vestibular sides.
Tubes are welded into the lateral sections on both sides, into which rods are inserted to connect with the head bandage. TO
deficiencies of the dentogingival
tires should include bulkiness, overlap of the mucous membrane of the alveolar process and hard palate, the need to obtain a complete impression from the upper jaw, weak fixation of the fragment. In order to eliminate shortcomings
Z.Ya. Schur proposed to replace the Weber splint with a single brazed splint with tetrahedral tubes in the lateral sections to strengthen the extraoral rods in them. The outer ends of the rods are rigidly connected to the gypsum cap with counter rods extending vertically down from the gypsum cap.
In the treatment of a simultaneous fracture of the upper and lower jaws, a periodontal splint with extraoral rods is indicated.
- with a mustache and toe hooks for intermaxillary fixation of fragments of the lower jaw, fixed to a soft head cap, proposed by A.A. Limberg.
With timely immobilization of jaw fragments with non-gunshot fractures, they grow together after 4
-
5 weeks Usually after 12
-
15 days after the injury, primary callus can be detected along the fracture line in the form of a dense formation. The mobility of bone fragments is markedly reduced. By the end of 4
-5th week, and sometimes even earlier, the mobility of fragments disappears with a decrease in compaction in the fracture area
- secondary callus is formed.
In X-ray examination, the gap between the bone fragments can be determined up to 2 months after the clinical healing of the fracture.
Therapeutic splints can be removed after the disappearance of the clinical mobility of fragments. The healing time for gunshot fractures is significantly increased.
Comprehensive restorative treatment of fractures is carried out under the control of radiography, myography and laboratory research methods.
12.2. CLASSIFICATION OF COMPLEX jaws
-
FACIAL DEVICES
Fastening of fragments of the jaws is carried out using various orthopedic devices. All orthopedic devices are divided into groups depending on the function, area of fixation, therapeutic value, design, manufacturing method and material.
By function:
- immobilizing (fixing);
- reponing (correcting);
- corrective (guides);
- forming;
- resection (replacing);
Combined;
- prostheses for defects of the jaws and face.
Place of fixation:
- intraoral (single jaw, double jaw, intermaxillary);
- extraoral;
- inside
- and extraoral (maxillary, mandibular).
For medical purposes:
- basic (having independent medical value: fixing, correcting, etc.);
- auxiliary (serving for the successful implementation of skin
- plastic or bone
- plastic surgery).
By design:
- standard;
- individual (simple and complex).
According to the manufacturing method:
- laboratory production;
- non-laboratory production.
According to materials:
- plastic;
- metal;
- combined.
Immobilizing devices are used in the treatment of severe fractures of the jaws, insufficient number or absence of teeth on fragments. These include:
- wire tires (Tigerstedt, Vasiliev, Stepanov);
- tires on rings, crowns (with hooks for pulling fragments);
- tires
- kappas:
V metal
- cast, stamped, soldered;
V
plastic;
Removable tires Port, Limberg, Weber, Vankevich, etc.
Repositioning devices that promote the reposition of bone fragments are also used for chronic fractures with stiff jaw fragments. These include:
- repositioning devices made of wire with elastic intermaxillary traction, etc.;
- devices with inside
- and extraoral levers (Kurlyandsky, Oks
- mana);
- repositioning devices with a screw and a repulsive platform (Kur
- Landsky, Grozovsky);
- repositioning apparatus with a pelot on a toothless fragment (Kurlyandsko
- go, etc.);
- repositioning devices for edentulous jaws (Guning splints
-
port).
Fixing devices are called devices that help hold fragments of the jaw in a certain position. They are subdivided:
- for extraoral:
V standard chin sling with head cap;
V standard tire according to Zbarzh and others.
- intraoral:
■V
tooth splints:
wire aluminum (Tigerstedt, Vasiliev, etc.);
brazed tires on rings, crowns;
plastic tires;
fixing dental devices;
■
tooth-gingival tires (Weber and others);
■
gum tires (Port, Limberg);
- combined.
Guides (corrective) are called devices that provide a certain direction to the bone fragment of the jaw with the help of an inclined plane, pilot, sliding hinge, etc.
-
For wire aluminum tires, the guide planes are bent simultaneously with the tire from the same piece of wire in the form of a series of loops.
-
For stamped crowns and mouth guards, inclined planes are made of a dense metal plate and soldered.
-
For cast tires, the planes are modeled from wax and cast along with the tire.
-
On plastic tires, the guide plane can be modeled simultaneously with the tire as a whole.
-
In case of insufficient number or absence of teeth in the lower jaw, splints are used according to
Vankevich.
Forming devices are called devices that are the support of plastic material (skin, mucous membrane), create a bed for the prosthesis in the postoperative period and prevent the formation of cicatricial changes in soft tissues and their consequences (displacement of fragments due to constricting forces, deformations of the prosthetic bed, etc.). By design, the devices can be very diverse, depending on the area of damage and its anatomy.
- physiological features. In the design of the forming apparatus, a forming part and fixing devices are distinguished.
Resection (replacement) devices are called devices that replace defects in the dentition formed after the extraction of teeth, filling defects in the jaws, parts of the face that arose after trauma, operations. The purpose of these devices
- restore the function of the organ, and sometimes keep fragments of the jaw from displacement or soft tissues of the face from retraction.
Combined devices are called devices that have several purposes and perform various functions, for example: fixing fragments of the jaw and forming a prosthetic bed or replacing a defect in the jawbone and simultaneously forming a skin flap.
A typical representative of this group is kappovo
- rod apparatus of combined sequential action according to Oxman for fractures of the lower jaw with a bone defect and the presence of a sufficient number of stable teeth on fragments.
Prostheses used in the maxillary
- facial orthopedics, divided into:
- on dentoalveolar;
- jaw;
- facial;
- combined;
- during resection of the jaws, prostheses are used, which are called post-resection prostheses.
Distinguish between immediate, immediate and distant prosthetics. In this regard, the prostheses are divided into operational and postoperative. Replacement devices also include orthopedic devices used for palatal defects: protective plates, obturators, etc.
Prostheses for defects of the face and jaws are made in case of contraindications to surgical interventions or in case of persistent unwillingness of patients to undergo plastic surgery.
If the defect captures a number of organs at the same time: nose, cheeks, lips, eyes, etc., a facial prosthesis is made in such a way as to restore all the lost tissues. Facial prostheses can be fixed with spectacle frames, dentures, steel springs, implants, and other devices.
12.3. TREATMENT TECHNIQUE FOR RIGID FRAGMENTS
A simple specialized treatment of mandibular fractures with limited mobility and stiffness of fragments is carried out by various devices that are well fixed on the jaw and have sufficient resistance to muscle traction. Limited mobility of fragments is observed when first aid is not provided in time or is carried out incorrectly. If the patient asked for help after 2
-
3 weeks after the fracture, the position of the fragments is almost always incorrect.
With single fractures with horizontal displacement of fragments to the midline, the most common, as well as for the treatment of fractures with freely movable fragments, are S.S. tires. Tigerstedt with hook loops.
In case of fractures within the dentition with stiff fragments, splints are made with hook loops on the upper jaw and a large fragment of the lower jaw, rubber traction is installed, and on a small fragment between the teeth
- antagonists place a gasket to squeeze it out. After a stable comparison of the fragments, the splint is removed and the treatment is completed with a single smooth splint. In some cases, it is advisable to leave the free end of the wire in the area of a small fragment, and after correcting the position of the fragments, it is bent to the teeth of a small fragment and fixed with a ligature.
With bilateral and multiple fractures, along with Tiger splints
- stadt shows tires with vertical P
- and G
- figurative bends, to which fragments are pulled with ligatures. In case of fractures of the lower jaw with a shortened dentition or in the presence of an edentulous fragment, Tigerstedt splints with hook loops are applied to the large fragment and the upper jaw, and a pelot is made on the edentulous fragment. In case of fractures behind the dentition, Tigerstedt tires with intermaxillary traction are applied, which are retained even after correcting the position of the fragments.
In this case, the appointment of myogymnastics is mandatory.
For the treatment of single fractures and fractures with a bone defect in the anterior section, the A.Ya. Katz with intraoral springy levers. It consists of supporting elements
- kappa or crowns, to which a flat or quadrangular tube is soldered from the vestibular side, and two rods. The advantage of the Katz apparatus is that it is possible to move fragments in any direction: parallel expansion or convergence of fragments, movement of fragments in the sagittal and vertical directions, expansion or displacement only in the region of ascending branches and angles of the jaw, rotation of fragments around sagittal (longitudinal) axes.
With a complete detachment of the upper jaw with stiff fragments (subba
- hall fracture) with posterior displacement and rotation around the transverse axis for simple specialized treatment, traction is applied to the rod, reinforced to the plaster cast. The rod is made of steel
wire, its free end ends with a loop. A wire splint with hook loops is placed on the teeth of the upper jaw. By means of rubber traction, the displaced jaw is pulled to the lever fixed on the headband.
With a unilateral complete separation of the upper jaw, when a sufficient number of teeth have been preserved on both jaws, the reposition of the stiff fragment is achieved by intermaxillary traction. A splint with hook loops is placed on the lower jaw, and the upper splint is attached only on the healthy side, where the hook loops are made. On the affected side, the end of the tire is smooth and remains free. Rubber traction is applied between the toe loops, and between the teeth on the side of the fracture
- elastic lining. After the reposition of the fragment, the splint is fixed to the teeth of the diseased side.
12.4. ORTHOPEDIC TREATMENTS FOR FALSE JOINTS
To the consequences of the maxillofacial
- facial injuries also include ununited fractures of the jaws or a false joint (pseudoarthrosis). The most characteristic sign of an ununited fracture is the mobility of the jaw fragments. During the Great Patriotic War, about 10% of mandibular fractures ended in the formation of a false joint. These were fractures predominantly with a bone defect.
Wire tooth splints by S.S. Tigerstedt. (1916)
There are five main types of these tires: a) a smooth tire-bracket, b) a tire with a spacer bend, c) a tire with hook loops, d) a tire with an inclined plane, e) a tire with a supporting plane. For the manufacture of dental splints, you need: aluminum wire with a diameter of 1.8-2.0 mm and a length of 12-15 cm or stainless steel wire with a diameter of 1.3-1.5 mm, a bronze-aluminum ligature wire with a diameter of 0 is used to fix the tires .5-0.6 mm or polyamide thread. The disadvantage of wire tooth splints is the impossibility of using them in case of a deep bite with a vertical or retrusion position of the teeth.

Indicationsfor use:
unilateral linear fracture of the lower jaw, located within the dentition, without displacement or with easily reducible fragments within the frontal group of teeth;
fractures of the alveolar part of the lower jaw and the alveolar process of the upper jaw;
fractures and dislocations of the teeth, when there are stable teeth on both sides of the intact areas of the jaw;
splinting of teeth in acute odontogenic osteomyelitis and periodontitis.
for the prevention of a pathological fracture of the lower jaw, before performing sequestrectomy, cystectomy, cystotomy, resection of a part of the jaw, etc.;
incomplete fractures (cracks) of the lower jaw.

Indicationsfor use:
Unilateral fracture of the lower jaw without displacement or with easily reducible fragments, if the fracture gap passes through the alveolar part, devoid of teeth.
3 .Tire with toe loops.
.Tire with toe loops.
Indicationsfor use:
mandibular fractures outside the dentition;
fractures of the lower jaw within the dentition in the presence of 4 on a larger fragment, and 2 stable teeth on a smaller one;
mandibular fractures with difficult-to-reset fragments that require traction;
bilateral, double and multiple fractures of the lower jaw;
fracture of the upper jaw (with the obligatory use of a chin sling);
simultaneous fractures of the upper jaw and lower jaw (complemented with a chin sling).
4 .
Tire with an inclined plane.
.
Tire with an inclined plane.
Indicationsfor use:
with significant defects of the lower jaw as a result of traumatic osteomyelitis, a gunshot wound or after operations for resections. Prevents displacement of the fragment towards the oral cavity, setting it in the correct articulatory relationship with the opposite dentition.
2) fractures in the region of the ascending branch.
5
 . Tire with holding plane.
. Tire with holding plane.
Indicationsfor use: on the upper jaw to hold tampons, soft tissue flaps of the palate in case of damage or in the postoperative period.
M  Method Betelman A.I. and Fidel M.P.
Method Betelman A.I. and Fidel M.P.
The method is a modification of the Tigerstedt method.
On the upper jaw, a tire with hook loops is strengthened; on each fragment of the lower jaw, rubber rings are tied to 1-2 teeth with a ligature and put on the loops of the upper splint. Thus, the displaced fragments are set in the correct position. After that, a wire splint with hook loops is bent for the entire dentition of the lower jaw, the elastic bands are removed, several wire ligatures are passed between the teeth on the fragments of the lower jaw, and the finished splint is attached to the teeth, performing double-jaw splinting according to the Tigerstedt method.

Tire V.A.Entelisa (twisted tire-spacer)
Indications: fractures of the lower jaw with a defect in the bone tissue in the frontal section.
Steel tire 3. N. Pomerantseva-Urbanskaya(three options).



an arc that moves a toothless fragment downward with the help of a pelota;
an arc that moves the fragment downward in the presence of stable ones;
an arc with a spacer in the presence of a bone defect.
The tire is made of stainless steel wire with a diameter of 1.3-1.5 mm. The bending technique is the same as for bending aluminum wire. Shown in cases where the strength of the aluminum tire is insufficient. This splint can be used not only for fixation, but also for repositioning of jaw fragments, and due to its strength, indications for the use of a single-jaw splint can be expanded.
W  ination according to G.V. Kruchinsky and S.I. Subotko (1989).
ination according to G.V. Kruchinsky and S.I. Subotko (1989).
A distinctive feature of this type of splinting is the use of the laws and rules of biomechanics in maxillofacial traumatology, which lie in the fact that the main stress trajectories, according to the authors, run along the lingual surface of the body of the lower jaw. Thus, it is more rational to place the wire splint on the lingual surface of the teeth. The tire is fixed with a ligature wire to each tooth, then hook T-shaped hooks for intermaxillary traction are formed from the ligature wire, brought out in the vestibule of the oral cavity.
Indications for use: fractures of the lower jaw with a sufficient number of stable teeth on fragments (the method is especially effective for fractures of the chin section of the lower jaw).
W  inirovanie according to P.I. Popudrenko and A.I. Stepanov.
inirovanie according to P.I. Popudrenko and A.I. Stepanov.
Intermaxillary traction according to P.I. Powdering is carried out with the help of rubber rings, on which two S-shaped hooks made of steel (stainless) wire are put on. One of the hooks is fixed to a smooth wire maxillary splint, and the other is fixed to the same mandibular splint. A.I. Stepanov puts on a smooth bus-bracket to put on special, pre-prepared flat hooks made of brass, stainless steel or duralumin. They move freely along the tire and, as it is fixed, are installed in the necessary places between the ligatures.
Indications for use the same as for the Tigerstedt bus.
Double tire Bader I.Ya. The method of fixing it to the teeth is facilitated, it holds fragments well, since it is double - on the vestibular side, the teeth are fixed by a Tigerstedt splint with hook loops, and on the oral side - by a wire ligature.
but  ) Tigerstedt's vestibular splint fits snugly to the dentition. Its free end is bent in the form of a loop, through which a ligature is passed, both ends of it are placed on the lingual side of the teeth, they are brought out into the gap between the canine and the lateral incisor.
) Tigerstedt's vestibular splint fits snugly to the dentition. Its free end is bent in the form of a loop, through which a ligature is passed, both ends of it are placed on the lingual side of the teeth, they are brought out into the gap between the canine and the lateral incisor.
b) the tire is fixed with a direct nodal tie.
 Splinting according to the method of A.P. Vikhrov and M.A. Slepchenko
Splinting according to the method of A.P. Vikhrov and M.A. Slepchenko
It consists in the fact that a bronze-aluminum ligature is fixed on the dentition with a polyamide thread from the lingual side, and itself, in turn, fixes an aluminum splint (smooth or with hook loops) from the vestibular side.
W  ination according to the method of P.Z. Arzhantsev.
ination according to the method of P.Z. Arzhantsev.
It consists in the fact that smooth tooth wire splints are fastened with polyamide thread, thus eliminating the need for hooks or loops.